Introduction
It is known that facial prostheses, such as ear prosthetics, made of wax, were used in ancient Egypt.
The first historical evidence of the use of facial prostheses dates back to the sixteenth century: the French surgeon Ambroise Paré describes the first artificial nose made of gold, silver and papier-mâché, which was attached to the face using a headband. In the second half of the 19th century, Claude Martin put forward the idea of creating an immediate denture using the tissues of the upper and lower jaws as a matrix to create complex structures. In the 20th century, with the advent of silicone materials, the quality and realism of craniofacial prostheses improved significantly, but the problem of fixation, which affects the appearance, function of the prosthesis, and patient comfort, was not completely solved. With increasing aesthetic demands, traditional fixation methods such as adhesives, pockets, loops and glasses have become unacceptable. In 1997, Brånemark installed the first bone-anchored extraoral hearing aid implant, and in 1979 the bone-anchored ear prosthetic implant. These events changed the entire concept of maxillofacial prosthetics. Since then, extraoral bone implants have been widely used to support prosthetic eyes, ears, and noses. Their use partially solves the problems of discoloration and deterioration of the prosthetic material, since these problems are often associated with adhesive materials. The skin and mucous membranes are less irritated by the mechanical effects of permanent fixatives and the chemical effects of adhesives and solvents. Implant-retained craniofacial prostheses have improved significantly from an aesthetic point of view due to their ease of installation, as well as thinner edges that blend in color with the skin. A large number of scientific and clinical studies confirm the success of their use and note an improvement in the quality of life of patients. Facial injuries and mutilations, especially after radical surgery, often lead not only to external physical disabilities, but also to functional and psychological disorders. In such cases, maxillofacial surgeons and dental prosthetists have to carry out a whole range of rehabilitation procedures. The options for reconstructive plastic surgery are often limited due to unfavorable conditions, such as damage to the vascular system of the surgical site due to radiation therapy, or insufficient volume of residual soft and hard tissue. In such cases, rehabilitation of patients with severe craniofacial defects is carried out with the help of prostheses, which represent an acceptable solution from an aesthetic point of view. A facial prosthesis is created by a craniofacial surgeon, maxillofacial orthopedist and prosthetic technologist as a good alternative to reconstructive surgery. To replace missing hard and soft facial tissues, prostheses using extraoral implants with a ball abutment, a bar design, or a choice of magnetic abutment are used. The shape of the prosthetic nose, eyes and ears, its color and texture should, as far as possible, be indistinguishable from the surrounding natural tissues. Rehabilitation can only be successful when patients are able to appear in public without attracting unwanted attention. Extraoral implants have many advantages in correcting facial defects over both adhesive prostheses and spectacle-mounted prostheses. They are characterized by ease of fixation of the prosthesis, which ensures the ability to properly install the prosthesis, thereby promoting comfort and confidence in its use. There is no skin irritation from the adhesive, and there is no need to wash off the adhesive every time after using the prosthesis. A thinner denture can be made, with thinner edges that blend into the skin, improving the overall appearance. During preoperative planning, when meeting with the patient, specialists from various fields not only show him the options for prostheses, but also teach him how to care for the abutment and prosthesis.
Implants have played a critical role in improving patient acceptance of facial prostheses. Patients enjoy the safety, comfort, and convenience of implant-supported dentures—benefits previously unattainable with older fixation methods. Over time, surgeons have noted a decrease in the number of patients requiring multiple complex surgical procedures. When correcting large defects, a combined approach combining tissue grafting and prosthetics using implants is recommended to achieve optimal results.
A three-implant facial prosthesis is the preferred method of replacing missing hard and soft orofacial tissue. Fixation on extraoral implants stimulates more confident behavior of the patient in public. Multidisciplinary treatment will require the combined efforts of several specialists. If we are talking about a defect in the eye socket, then the efforts of an ophthalmologist, a craniofacial surgeon, a maxillofacial orthopedist and a prosthetic technician are required.
Midface defects can be divided into two broad categories: midline midface defects, which include the nose and/or upper lip, and lateral facial defects, which include the cheeks and orbit.
The choice between plastic surgery and a prosthesis for serious facial injuries remains difficult and depends on the area and etiology of the damage, as well as on the wishes of the patient. The development and use of extraoral implants for the correction of facial defects has to some extent changed the attitude of patients towards facial prostheses. Implants provide comfortable donning and reliable fastening of the prosthesis, which improves the perception of the prosthesis by patients.
We will conduct a retrospective review of patients who underwent facial prosthetic reconstruction from 2005 to 2010. Clinical reports describe step by step the materials and methods used, including the implant procedure.
There are three main diagnoses that require surgical intervention: oncological, traumatological and genetic and/or acquired diseases. The goals of surgical and prosthetic rehabilitation are to replace missing hard and soft facial structures, restore physical impairments, alleviate social problems and improve quality of life.
Treatment protocol
Treatment of a patient with oral cancer or after trauma is a collaborative effort between craniofacial surgeons, oncologists, radiation therapists, and prosthetic technicians.
Typically, immediately after radical surgery, a free tissue graft is performed to restore both soft and bone tissue. A large percentage of patients receive 4 to 6 weeks of radiation therapy after surgery. The total radiation dose to the tumor bed depends on the presence or absence of cancer cells at the surgical margin of the tumor. The radiation dose usually does not exceed 55 Gy, for cases with a clear pathological margin, and from 65 to 70 Gy, with a narrow pathological margin. Radiation localizers are widely used, and radiation fields are adjusted in such a way as to minimize the possibility of large salivary glands entering the area of exposure to large doses of radiation; however, intensity-modulated radiation therapy was not used. Radiation dose to bone can often be minimized in areas where implants are to be placed. Approximately 6 weeks after radical surgery, the patient was expected to undergo radiation therapy for 5 to 7 weeks. Once the patient had recovered from plastic surgery and radiation therapy, new standard prostheses were made. The implants were planned to be placed 4-6 weeks after plastic surgery, depending on the need for post-operative radiation therapy. All implants were placed based on wound healing from osteotomy and recovery from radiation therapy. Three implants were installed. The implants were installed in the existing native bone tissue and/or in the free vascularized bone tissue of the reconstructed mandible. During the operation, before installing the implants, excess plate segments were removed to connect the bone fragments.
Prosthetic options include classically anchored dentures, then implants with ball-shaped attachments, bar structures and magnets.
The long-term prognosis is important, but having a high-quality prosthesis for even a year or two can significantly improve a patient's quality of life. The advantage of installing implants and facial prostheses is that the perfect stability of the prosthesis guarantees the patient's return to social life.
External changes in the lower third of the face
Asymmetry - how to correct the situation?
Most radical and “global” rejuvenation treatments affect the lower third of the face. Why? The answer is quite simple: it is in the lower third of the face that the dentofacial system is concentrated, which, for a number of reasons, undergoes significant changes, leading to changes in the surrounding facial tissues. The process, if described in simple words, looks like this: the bone atrophies, the tissue follows the bone. Visually, this violates the aesthetics of the face, causing facial asymmetry.
The presence of bite pathologies can also affect facial aesthetics
.
Let's look at it in order:
First, as it happens, one tooth is lost
.
Missing one tooth. Starting factor #1
If only one tooth is missing, then at first it may not be very noticeable; the contour of the lips will change slightly, as the lip will begin to “sink” into the place of the missing tooth.
But there is one important point: the bone tissue in the absence of a tooth will begin to dissolve.
What does this mean from the point of view of violation of facial aesthetics:
- The necks of neighboring teeth will gradually begin to become exposed and their loss may occur,
- in this case, the lip will sink even more, affecting the neighboring muscles, and small vertical folds may appear above the lip.
The loss of one tooth is not critical, but you need to know that as a result of the loss of a tooth in the chewing region, the load will begin to be redistributed to other teeth, including the anterior frontal region. And the additional, unplanned by Nature, load on the teeth leads to their abrasion
. When two or more teeth are lost, the processes of distributing the load on adjacent teeth begin to occur more actively.
So, the next factor is tooth wear.
Tooth wear and bruxism. System factor #2
Now let's look at what happens with tooth wear and bruxism.
At its core, tooth wear involves abrasion of the tooth tissue. With pathological abrasion and bruxism, this process occurs many times faster, the crown part of the tooth decreases, and again the height of the lower third of the face decreases.
When teeth wear down, changes occur in the temporomandibular joint, just as in the absence of teeth.
What aesthetic defects
faces appear when erased:
- the lower jaw gradually begins to rise upward,
- the distance between the tip of the nose and the chin decreases,
- nasolabial folds increase,
- Vertical wrinkles appear around the lips.
The next factor in external aesthetic changes in the face is malocclusion
. This is one of the most common problems.
Malocclusion. Global factor #3
If the teeth are not positioned visually, it may:
- the tip of the chin moves,
- a second fold appears under the chin,
- “cluttered” chewing teeth can externally “round” the jaw line at their location, that is, the jaw line from the chin towards the ear will not be “chiseled”.
- also, if the teeth are incorrectly positioned, the lower jaw can protrude forward or, on the contrary, move backward - outwardly such a chin looks “sloping”, as if the neck immediately begins from the chin.
Bite pathology very often “adds” a sufficient number of unplanned wrinkles
.
From an aesthetics point of view, a problem arises that very often begins to be solved with the help of cosmetic procedures: Let’s look at what it looks like using specific examples of only two malocclusion pathologies (and there are many more of them).
Did you know that, for example, the feature of the distal occlusion
is there an imbalance in jaw development?
The teeth of the upper jaw quickly begin to protrude above the lower ones, while the lower jaw lags behind in development, as a result of which the chin appears small and looks unnatural. From an aesthetic point of view, this leads to the appearance of wrinkles
in the lip area. And the face itself becomes unattractive.
And in case of deep bite
there is a significant overlap of the lower dentition with the upper teeth and, as a consequence of such contact, there is increased wear of the teeth, which we talked about earlier in factor #2, which further leads to a reduction in the lower third of the face.
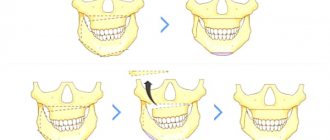
We started the story with factor #1 - the loss of one tooth. But the most serious problems of facial aesthetics begin with the loss of several teeth, when bone tissue atrophy begins to develop, entailing, in fact, both bone atrophy and changes in the structure of soft tissues.
So - edentia. Global factor #4
Adentia can be either complete or partial. With complete edentia, there is a complete absence of teeth on one or both jaws. Partial edentia implies the absence of one or two teeth or a segment of teeth, for example chewing teeth. Loss of teeth, especially complete loss, immediately affects the appearance of the face.
If teeth are missing, the height of the lower third of the face decreases, what does this lead to? This leads to a loss of support for the jaws by the teeth, as a result of which the jaw moves backward in the joint area, and forward and upward in the chin area. This is how an “old man’s face” appears - the distance between the tip of the nose and the top of the chin decreases.
How does edentia appear on the face?
What aesthetic defects appear on the face during the development of edentia:
- all folds naturally begin to deepen, nasolabial folds become pronounced - they descend to the corners of the lips,
- the lips outwardly look much thinner, since when they lose support from the teeth, they shift towards the oral cavity,
- the tone of facial muscles decreases, the cheeks and chin tissues sag,
- in the absence of a group of chewing teeth, the soft tissues begin to “fall” inward.
- and with a long-term absence of chewing teeth, bone tissue begins to dissolve, outwardly it looks like very “sunken cheeks.”
As you can see, all these factors influence changes in the appearance of the face, its shape and gives asymmetry. Changes can occur regardless of age, but at the same time they make the face look older due to the deepening of the nasolabial folds and incorrect position of the jaws.
Features of designs with sticking effect
Various materials are used today to make removable dentures. The most budget option is regular plastic or acrylic. It is quite functional, but contains a monomer, so it can cause allergies. Orthopedic products made from monomer-free materials - acry-free, dental nylon, polypropylene - do not have this drawback.
New generation removable dentures with an adhesive effect are equipped with a silicone insert between the base of the structure and the gum. This layer helps distribute the load more evenly when chewing food. In addition, the silicone insert improves the fixation of the prosthesis on the upper or lower jaw, due to the suction effect and a very precise fit. Such designs are created individually for each patient, taking into account the anatomical features of the jaw.
What does cosmetology offer for facial rejuvenation?
Now that you have understood the basics of dental pathologies that affect the appearance of the lower third of the face, let's look at the main range of cosmetic procedures that are aimed at maintaining facial tissue and skin in tone and which have an externally rejuvenating effect.
Let us immediately make a reservation that most of these procedures do not have a permanent effect, and in order to always look young (not only in the soul, but also in appearance), these rejuvenation procedures must be repeated regularly.
So, modern rejuvenation methods guard your beauty
Face lift
Let's look at several options for procedures for correcting the lower third of the face and eliminating asymmetry.
Lipolitics
The procedure for modeling the face using lipolytics is called injection lipolysis. Lipolitics are preparations based on natural ingredients, their main action is aimed at the breakdown of subcutaneous fat cells, resulting in a rejuvenating effect.
The effect of the procedure with lipolytics occurs quite quickly, the oval of the face changes, and the subcutaneous tissue structure is aligned. The procedure does not allow the splitting of an extensive layer of fat.
In what cases are lipolytics used?
- if you need to eliminate a double chin,
- form a natural oval face,
- reduce the volume of the cheeks,
- eliminate defects in the shape of the nose,
- correct nasolabial folds
Cost per 1 ml
procedures vary
from 3 thousand rubles
and more, depending on the drug, the number of milliliters administered and the number of correction zones. For a pronounced effect, you need at least six to eight procedures for each zone, which involves serious expenses, reaching 200 thousand rubles and even higher.
The lifting effect is temporary. After some time, the procedure is usually repeated.
Mesotherapy
Mesotherapy consists of therapeutic injections of individually selected cocktails, which are injected into the middle layer of the skin with a very thin needle.
After the mesotherapy procedure:
- complexion improves,
- muscle tone increases,
- you can eliminate “creases” in the skin,
- you can remove nasolabial folds and drooping corners of the lips,
- You can remove your double chin.
The number of rejuvenating procedures during mesotherapy depends on the age and problems that need to be eliminated. Mesotherapy has a cumulative effect, the results of the procedures can be seen in 2-4 weeks. On average, 5 to 7 procedures are required with an interval of 1 time per week; if necessary, the cosmetologist can increase the number of mesotherapy procedures. The cost of the procedure varies from 4000 - 5000 rubles
and higher in one procedure.
Mesotherapy effect
- temporary. To maintain the effect, the procedure must be repeated once every 6-12 months.
Biorevitalization - 3D face lifting with hyaluronic acid
The biorevitalization procedure is currently the most popular. We all know well, according to doctors, that the main property of hyaluronic acid is to retain moisture, maintaining the natural hydrobalance of the skin.
Biorevitalization is carried out in all areas where there are problems - on the face, neck, décolleté, and is also used in other areas of the body, providing the necessary hydro reserve to the skin layers. Injection biorevitalization is comparable in effect to a surgical facelift; the procedure can completely sculpt the face.
Using hyaluronic acid injections, you can correct the lower third of the face:
- remove pronounced nasolabial folds,
- remove flaws, if any, on the chin, that is, change its shape,
- and also adjust the profile along the lower jaw.
Cost of biorevitalization.
The cost of injections depends on the drug used, its density and the number of milliliters required for the procedure. For example, for visual correction of malocclusion (the area under the chin), you may need up to 4 ml of the drug, the cost of 1 ml is from 18-20 thousand rubles. The general course can range from 1 to 5 procedures at intervals.
The effect of biorevitalization
- temporary. After the procedure, there is an immediate, pronounced visual effect that lasts from 5 to 12-15 months; to maintain the effect, the procedure must be repeated.
Kogi threads
Cog mesothreads provide a clear oval face and a pronounced lifting effect. Installed mesothreads contribute to the formation of dense connective tissue, and also help to activate the production of collagen and elastin, which are responsible for skin elasticity.
Kogi threads have notches, thanks to which it is possible to achieve:
- pronounced lifting effect,
- clear contour, tightening of soft tissues and prolonged action of thread lifting,
- They perfectly hold the given shape of problem areas of the face or body.
You may need 4-6 threads for the whole face, the average price is from 5 - 15 thousand rubles for 1 thread.
Effect of the procedure
- longer lasting, but also temporary. Kogi threads have a prolonged effect, the result of the procedure lasts from 2 to 4 years, to maintain the effect the procedure must be repeated.
Nasal prosthesis
Clinical report
A 63-year-old woman diagnosed with recurrent basal cell carcinoma of the nose was treated.
After nasal amputation, external beam radiation therapy and chemotherapy were performed. Oncological treatment was completely completed in 2007. Surgical restoration and installation of the prosthesis began a year after the end of treatment (Fig. 1, 2). Three extraoral implants were inserted along the edge of the postoperative defect. The operation was performed under general anesthesia with nasopharyngeal intubation. The main implant bed for the nasal prosthesis was a pear-shaped ridge at the base of the nose (2 implants - left and right). The other bed was the glabella; we paid special attention to the degree of pneumatization of the frontal sinus and the amount of overlying bone tissue. The operation lasted 65 minutes and went without complications. The wound healed without inflammation. Lincomycin (600 mg orally) was used as an accompanying antibiotic. Four days after the operation, the patient was discharged in good condition. Six months after the installation of the implant and the end of the healing period, prosthetics began. A control tomogram was performed. Magnetic mounts were inserted. The prosthesis was prepared as follows. A one-stage prosthetic technology was used; a nasal prosthesis with separately located abutments and magnetic fixation was chosen. It was investigated in which direction the protruding parts of the abutments are directed. It was required that the fixation elements be oriented so that the prosthesis would extend beyond the anterior edge of the maxillary bone. To achieve this and position the fixation components in a position that is easy to manipulate, cantilever abutments were chosen. An additional set of magnetic abutments was ordered to select the appropriate cantilever angle.
The defect impression is recorded as a partial alginate impression. A plaster model of the prosthetic element was made. Base wax was used to sculpt the edges of the acrylic resin base. The wax-up model was prepared, evaluated on the patient and brought to its final form.
The plaster mold is cast. The wax is melted out, and the surface of the plaster model and casting mold is coated with a release agent and auto-polymerizing acrylic plastic. Acrylic plastic is subjected to pressure treatment in a polymerizer. The shape of the prosthesis, its color and texture are finalized using special plastic. The finished prosthesis is ground and polished. A magnet is attached to the top of the support. An impression is made of the contact surface between the abutment and the fixture using single-phase silicone. Magnets connect to the abutments.
Figure 1. Nasal prosthesis: a) wax cast; b) polymerization; c) coloring; d) installation of magnets.
Figure 2. Nasal prosthesis: a) CT scan after installation of 3 implants, b) magnetic attachments; c) patient after rehabilitation.