- Surgical department
Surgical department » - Maxillofacial Surgery
Maxillofacial Surgery "
- Jaw osteotomy
Malocclusion is a violation of the process of chewing food and swallowing it, a negative effect on the speech apparatus, as well as an aesthetic defect. With malocclusions, the upper and lower jaws can be enlarged or reduced in size, pushed forward or positioned posterior to the normal position, shifted to the side or tilted, turning clockwise or counterclockwise. In this case, the closure of the teeth is disrupted to one degree or another, they change the angle of inclination, turn around, run into each other (crowding) or diverge with the formation of cracks (treme).
What are the dangers of malocclusion?
- Violation of dental contacts makes it difficult to chew food and provokes the development of diseases of the gastrointestinal tract.
- Severe malocclusions so limit the possibilities of normal nutrition that they are a reason for deferment from the army.
- Changing the angles of inclination of the teeth affects the distribution of the load during chewing, leads to overload of the periodontium, the development of gum inflammation and, ultimately, earlier tooth loss.
- Teeth crowding, combined with misalignment, affects the natural cleaning of teeth, further leading to the development of gum disease and an increased likelihood of tooth enamel destruction. If tooth loss has already occurred, then violations of the jaw relationships can create difficulties in prosthetics.
- Malocclusion leads to a change in the trajectory of jaw movement during chewing: the temporomandibular joints are overloaded, and dysfunction of the temporomandibular joints develops.
- Some types of malocclusion are anatomical prerequisites for narrowing the airways, for the appearance of snoring and such a serious condition as sleep apnea.
Atrophy of the alveolar process. What it is?
Few people know that the volume of bone tissue is not a constant, and can change in the same way as the volume of muscle or fat tissue.
And just like muscle, bone tissue is sensitive to the existing load and atrophies with inactivity. Thus, when a tooth is lost, the jaw bone or alveolar process undergoes atrophy, loss of bone tissue. However, unlike muscle atrophy, bone atrophy of the alveolar processes is an irreversible process. Lack of timely assistance in the event of the loss of one or more teeth is fraught with the development of gum atrophy, frenulum deformation, malocclusion, diction and speech, and progression of facial asymmetry. When the process is neglected, the entire dentition becomes displaced and healthy teeth are damaged.
The longer a tooth or teeth are missing, the more noticeably the amount of bone tissue decreases, and the more difficult it will be to correct the problem. NKclinic undertakes surgical treatment of alveolar atrophy of any severity and severity. For our experienced specialists, leading maxillofacial surgeons, there are no impossible tasks. However, we nevertheless do not recommend that you delay treatment. Time is not on your side in this matter.
Jaw osteotomy surgery
Historically, the first operations were performed on the lower jaw. And the surgeon’s task was precisely to restore normal jaw relationships. But today operations on the lower jaw alone account for no more than 10% of operations performed. Because the surgeon’s tasks have changed: now it is not only the correction of the bite, but also the improvement of facial aesthetics.
Double-jaw osteotomy is an operation on the lower and upper jaw simultaneously, which allows you to achieve aesthetically favorable proportions of the face both in front and in profile, eliminate asymmetry, and make the smile brighter by eliminating dark corridors - shading of the lateral teeth of the upper jaw. We can say that surgery on one jaw is only a correction of functionality, on two – functionality and aesthetics.
Indications for the operation:
- violation of the closure of the dentition, which cannot be corrected orthodontically;
- pronounced facial disproportions that have aesthetic significance.
Contraindications:
- unpreparedness of the dentition for surgery (insufficient orthopedic or orthodontic preparation);
- diseases of internal organs that prevent surgery or anesthesia.
Methods of surgical treatment of alveolar process atrophy at NKclinic
The treatment strategy is determined individually for each patient. When choosing it, concomitant pathologies, both of the maxillofacial area and of a systemic nature, are taken into account, the data obtained as a result of computer diagnostics are carefully studied. First of all, our specialists take into account the duration of tooth loss and the severity of atrophy. At the initial stages - in the first 2-3 years after tooth loss - atrophy in thickness is observed. In such cases, surgeons choose one of the following operations:
- Guided bone regeneration (GBR). The volume of the bone is increased with the help of bone chips, both natural and artificial. It is pressed against the atrophied alveolar process with a biologically inert membrane with titanium pins or titanium mesh, or bone blocks taken from the lower jaw.
- Building bone mass with bone blocks. A bone fragment taken from the lower jaw is fixed to the affected area with titanium screws.
- Augmentation implantation. The complex operation is a one-stage plastic surgery with implantation. Dr. Nazaryan D.N., founder and leading specialist of NKclinic, first described this method in 2010. Previously, implantation was carried out no earlier than 4 months after bone grafting. Today, if primary fixation of implants and bone material is possible, we follow exactly this tactic. In this case, the period of complete healing is reduced by 6 months!
4-5 years after the loss of a tooth, wearing clasp dentures or systemic diseases affecting bone tissue, atrophy of the alveolar process occurs in height. This kind of problem can be solved with:
- Bone blocks, which are also transplanted from the lower jaw or from the parietal area. NKclinic was the first in our country to use the parietal bone graft technique. The only contraindication for this technique is the proximity of the mandibular nerve (less than 2 mm of bone tissue).
- Vertical osteotomy. The bone fragment of the alveolar process with the mucous membrane is sawed, lifted and fixed in a new place.
Stages of treatment
Today, the method of combined treatment of malocclusions, when the orthodontist begins work first, is considered generally accepted in the world.
1) Orthodontic stage
The orthodontist places braces on both jaws and begins to move the teeth so that they take the correct position in relation to the jaws. In this case, a temporary deterioration in the closure of teeth occurs. It takes about nine months to prepare. After this, the surgical stage is performed.
2) Surgical stage
The operation is performed under general anesthesia. The intervention is performed via intraoral access, which allows it to avoid leaving scars. In accordance with the treatment plan, cuts are made on the upper and lower jaws, the fragments are mobilized and installed in the most functionally and aesthetically advantageous position. Next, the jaws are fixed with titanium miniplates, which are invisible to the body, do not ring at the airport and do not interfere with MRI. They usually remain in the body for life without causing any consequences. In rare cases, surgery may be performed before orthodontic treatment begins.
Corrective osteotomy at the Ladisten clinic
The clinic specializes in minimally invasive orthopedic surgeries. More than 6,000 patients from all over the world have already undergone osteotomy and are satisfied. Each patient is offered a tour of the facility, a separate room during rehabilitation, and 24-hour medical supervision in the first days after the procedure. The operation itself is bloodless: a small puncture is made in the leg, through which doctors correct the bone. For fixation, a unique device from Dr. Veklich is used. This is an improved design of the Ilizarov apparatus. It is less bulky, weighs little and does not involve dangerous knitting needles. Doctors at the Ladisten Clinic have been performing corrective osteotomy procedures for more than 30 years; the price varies depending on the pathology and severity of the case. To find out the exact diagnosis, consult about contraindications and discuss the cost of osteotomy, just make an appointment by calling us at: +38 +38 or Write to WHATSAPP Write to VIBER We will choose a convenient time for you to visit the clinic or online consultation.
In the practice of surgical treatment of lower prognathism.
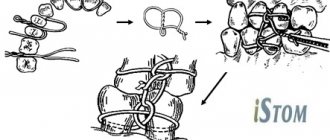
Or its combination with an open bite, horizontal osteotomy of the branches has found widespread use. Thus, A. A. Limberg (1928) performed this operation using a submandibular approach, performing an osteotomy slightly above the mandibular foramen. After moving the lower jaw into the correct position, the overhanging excess of the anterior edge of the upper fragment was removed. Fixation of the fragments was carried out with a wire suture and intermaxillary bimaxillary splints (Fig. 27).
This method is technically simple and has found wide application in the practice of other surgeons [AssM. S, 1931; Lando R. L., 1933; Rauer A.E., 1935; Rudko V.F., 1966; Yovchev V.S., 1967; Hogemann K. E., 1951; Rowe NZ, I960; Shira R.V., Ailing G.196I; Anastacov K., 1964; Gorski M., Tarezynska I.N., 1969, etc.].
M. Wassmund (1935) formed a spike-like protrusion on a small fragment, placing it in the corresponding notch on the outer compact plate of a large fragment of a branch (Fig. 28).
Y. Heiss (1957) made the spike on a small fragment longer, and the operation was completed with osteosynthesis with a wire suture. This surgical method was also used by other surgeons.
Methodology of V. S. Vasiliev
It differs in that after osteotomy and displacement of the lower jaw posteriorly, a small fragment of the branch is superimposed on the outer surface of the branch. The negative side of this modification is the creation of unfavorable conditions for consolidation due to the contact of fragments not with a spongy, but with a compact layer.
Most surgeons perform osteotomy on the mandibular branch not in an oblique, but in a vertical direction. In 1910, WW Babekosk performed a vertical osteotomy of the branches of the lower jaw, the line of which connected the middle of the semilunar notch with the angle of the jaw. After the lower jaw was displaced upward and an orthognathic bite was established, a wedge-shaped defect formed in the area of the osteotomy; the fragments were in contact in the upper section only in a small area, where osteosynthesis was carried out with a metal wire through two holes (Fig. 33).
Too small a contact area of bone fragments after osteotomy creates unfavorable conditions for consolidation, which makes the WW Babcock method one of the imperfect ones. This method continues to be used today [Tyukalov K.V., 1967; And rzhantse in P. 3. et al., 1970; Alekseev-L, I., 1970; Y. V. Caldwell, G. S. Zettermann, 1954; M. Robinson, 1954; Toman Y., 1958; Shira R.V., 1961; Ailing G., 1965: Ginestet G., Merville L., 1965, 1966; Constantinidis Y., 1967; BerenytB., 1968; KoppW.K., 1968, etc.).
In addition to the listed methods, some surgeons use vertical wedge resection on the branches of the lower jaw. Thus, Van Zile (1955) proposed an original method of triangular resection in the vertical direction of the branch using a submandibular approach. First, he performed a vertical osteotomy of the ramus from the middle of the semilunar notch to the corner of the jaw, and then shifted the medial fragment of the jaw posteriorly (or upward when prognathism of the lower jaw was combined with an open bite) until the correct bite was established. In this case, a small fragment of the ramus was superimposed on the branch, revealing the dimensions of the excess part on the large fragment, resected by the author in the form of a triangle, the apex of which faces the angle of the jaw, and the base faces the semilunar notch. The wound surfaces of the branch were compared end-to-end, and osteosynthesis was performed with metal wire (Fig. 34).
The advantage of this technique is that it allows you to increase the height of the jaw branch, reduce the angle of the jaw and preserve the neurovascular bundle. A similar technique, but with more accurate mathematical calculations and strong fixation, was carried out in 1966 by V. F. Rudko (Fig. 35).
In our practice, we have somewhat modified the vertical “sliding” osteotomy. In December 1966, patient S. underwent bilateral vertical “sliding” osteotomy of the branches of the lower jaw for lower prognathia of the second degree and an open bite of the first degree. After osteotomy and installation of the middle fragment of the jaw into the correct position, its excess was determined, since the small fragments were displaced onto the remainder of the branches of the large fragment. To eliminate excessive layering of branch fragments and improve their contact, we removed strips of the compact layer of branches from the outer surface of the large fragment and from the inner surface of the small fragment. The width of the strips was determined by the level of layering of small fragments. Thus, the exposed surface of the spongy substance of the branches had the shape of an inverted trapezoid. Fragments of branches were compared until complete contact of the spongy substance. Fixation was performed with two wire sutures (Fig. 36).
In the postoperative period, intermaxillary fixation was carried out for 37 days using dental wire splints and rubber traction. This operation achieved good cosmetic and functional results (Fig. 37-40).
Currently, planar osteotomies in the area of the angle and lower part of the mandibular ramus are quite widely used [Arzhantsev P. 3. et al., 1970; Mitrofanov G. G., Rudko V. V., 1972; Arzhantsev P. 3., Sukachev V. A., 1974; Sukachev V. A., Gritsai N. P., 1975, 1977; Rudko V.V., 1975, 1976; Semenchenko G.I., Lozenko P.A., 1975; Dal Pont, 1961; Obwegeser H., 1968; Tsvioro F., 1972, 1978, etc.].
The most successful and promising was:
Depending on the level and direction of osteotomy, there are:
Horizontal, oblique, vertical, arched, ledge-shaped, stepped, planar, etc. W. Lane in 1908 performed a horizontal osteotomy of the branches at the level of their middle third with damage to the neurovascular bundle using the submandibular approach. After the middle fragment of the jaw was shifted posteriorly to the correct position, the bone fragments were fixed with the author’s plate (Fig. 24).
In the postoperative period, intermaxillary fixation was carried out using naubal splints.
Ch. Bruhn (1920) and AL Zindemann (1921) abandoned the use of this plate. They fixed the jaw fragments only with the help of dental splints. They performed osteotomies of the branches of the lower jaw using a hacksaw through a preauricular incision.