Surgical removal of the parotid gland is called a parotidectomy . In most cases, surgery is performed due to the presence of a tumor, often benign, of the parotid salivary gland.
Parotid salivary gland and facial nerve - schematic drawing
The salivary glands secrete saliva into the mouth to digest food and protect against infections. When the parotid glands are removed, there are no problems with the secretion of saliva - this function will continue to be performed by the remaining salivary glands: the submandibular, sublingual, and numerous small glands.
The parotid gland is penetrated by nerves, veins and arteries. We are interested in the facial nerve.
Detailed description of the study
Salivary gland cancer is a malignant tumor of the salivary gland formed from epithelial cells. Tumors of the parotid salivary glands (PST) are a rare type of neoplasm. They mainly develop between the ages of 20 and 40. More common in men than in women. Tumors are usually located in the soft tissues of the face and often cause serious cosmetic defects, causing paresis of the facial nerve.
The main risk factors for developing salivary gland cancer are:
- Chronic inflammatory diseases of the oral cavity;
- Hormonal imbalances;
- Genetic disorders;
- Smoking;
- Nutritional factors (low vitamin content, high fat content in food).
Most often the tissues of the parotid salivary gland are affected - 80%, less often the tumor develops in the tissues of the submandibular salivary gland - 15%, sublingual or minor salivary gland.
The following options for the development of pathology are distinguished:
- Primary cancer (from the tissues of the gland itself);
- Secondary cancer (metastasis or germination from neighboring organs).
According to histological parameters, tumors of the salivary glands represent the most heterogeneous group of human neoplasms. More than half of them are benign formations.
Benign neoplasms of the parotid salivary glands are detected in more than 30% of patients who complain, malignant ones - in 65%. Among the morphological types of benign tumors of the parotid salivary gland, the most commonly diagnosed are pleomorphic adenoma (a benign formation that forms in the glandular epithelium), adenolymphoma, lipoma and a very rare adenoid cystic tumor (formed by epithelial cells lining the lumen of the gland).
Malignant tumor formations are most often represented by: mucoepidermoid cancer (formed by cells secreting mucus and epithelium) and adenocarcinoma. Acinic cell carcinoma also occurs, which mainly affects the tissue of the parotid salivary gland.
Usually, during examination of patients, palpation reveals a dense, painless formation in the area of the salivary glands, which, according to patients, grows generally very slowly. In approximately a third of cases, pain may be present.
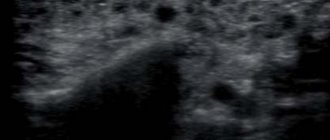
The “gold standard” for diagnosing tumors of the salivary glands is aspiration puncture of the tumor followed by histological examination of the obtained material, carried out before surgery or intraoperatively. The diagnostic value of this method is up to 90%, because the tissue of the affected area is studied directly under a microscope.
Aspiration puncture (biopsy) is performed using a special needle under ultrasound control. The study allows you to confirm or clarify the diagnosis, track the growth dynamics of the tumor and analyze the changes that occurred during tumor therapy.
During histological examination, three indicators are assessed:
- Tumor size and extent of its spread (T);
- The presence of damage to regional lymph nodes by metastases (N);
- Determination of metastases in other organs and tissues (M).
Based on the degree of malignancy, there are three types of tumors:
- High differentiation, when the cells are similar to glandular epithelial cells, such formations grow slowly and often have a favorable prognosis;
- Low differentiation, when cells are very different from normal, is characterized by rapid growth and early metastases;
- Medium differentiation.
Types and functions of salivary glands
Salivary glands are paired organs that differ in location:
- large parotid - located on the side of the lower jaw, under the left and right ears. They produce saliva containing high concentrations of potassium and sodium chlorides;
- large submandibular - adjacent to the lower jaw, have an excretory duct in the area of the lingual frenulum, produce saliva with a low acid index;
- large sublingual - located in the oral cavity under the mucous membrane, secrete alkaline saliva containing protein saturated with mucin (high molecular weight glycoproteins).
The minor salivary glands are located on the mucous membrane of the cheeks, lips, and tongue.
The role of the salivary glands is to secrete a fluid that contains special enzymes and is involved in the digestive process. They also perform the following functions:
- exocrine - production of proteins, fluids;
- endocrine - produce biologically active substances;
- excretory - participation in the removal of metabolic products from the body.
References
- Malignant tumors of the salivary glands, Clinical guidelines. Association of Oncologists of Russia, 2022. - 55 p.
- Balkanov, A.S., Bychenkova, O.A., Sipkin, A.M. and others. Combined treatment of parotid salivary gland cancer. Almanac of Clinical Medicine, 2022. - No. 4. - P. 309-313.
- Polyakov, V.G., Shishkov, R.V., Ermilova, V.D. and others. Children's Oncology, 2004. - No. 1. - P. 45-47.
- Carlson, E., Schlieve, T. Salivary Gland Malignancies. Oral and maxillofacial surgery clinics of North America, 2022. - Vol. 31(1). — P. 125-144.
Bougienage during examination of the salivary gland duct
Examination of patients with diseases of the salivary glands requires certain skills from the dentist, since often the first symptoms of this disease are inflammatory processes in the oral cavity.
After collecting anamnesis, visual and palpation examination, the following may be prescribed:
- sialometry using the Andreeva method - after making a bougienage into the duct of the salivary gland, a cannula (special tube) is inserted through which saliva is collected for quantitative and qualitative research;
- sialography (contrast x-ray diagnostics) - 1 - 2 ml of iodolipol or other iodine-containing substance, heated to a temperature of 37 - 40 degrees, is injected into the ducts of the salivary glands using a blunt needle. The mouth of the duct is first bougiened with a conical probe. An x-ray is taken immediately;
- pantomosialography (contrast x-ray diagnostics of several glands at once) - this procedure helps to determine the ongoing hidden inflammatory process of paired salivary glands, narrowing or widening of the ducts;
- digital (digital) subtraction sialography - performed with the introduction of a contrast agent.
Treatment
The patient is treated by a team of doctors, which may include: a clinical oncologist, an ENT doctor, an oncologist-surgeon, an oral and maxillofacial surgeon, a chemotherapist, a radiotherapist, etc. The treatment program is determined by the stage of cancer, the histological type of the tumor, its location (which gland is affected) , age, general condition and concomitant diseases of the patient.
Surgery
If the tumor has not grown much into the surrounding tissue, then it is resectable, that is, it can be removed surgically. The surgeon’s task is to excise the tumor while capturing the surrounding tissue so that there are no cancer cells left on the cut line, that is, to ensure a negative resection margin. If tumor cells have spread to the lymph nodes, or a biopsy reveals aggressive cancer, the lymph nodes are also removed.
For parotid salivary gland cancer, surgery presents certain difficulties, because the facial nerve passes through the gland, which controls the work of facial muscles. If the tumor affects only the superficial lobe of the gland, you can remove it separately - perform a superficial parotidectomy. There is no risk of damaging the facial nerve. In some cases, it is necessary to remove the entire gland, and if the tumor has grown into the facial nerve, then it too.
For cancer of the sublingual and submandibular gland, the surgeon removes the gland itself and some of the tissue located around it, including, possibly, bone tissue. In some cases, it is necessary to excise the nerves that control sensitivity, movements in the lower part of the face, in the tongue, and the sense of taste.
For cancer of small glands, the affected gland and part of the surrounding tissue are removed. The extent of the operation depends on the size and location of the tumor.
Radiation therapy
Indications for the use of radiation therapy for malignant tumors of the salivary glands:
- To combat malignant tumors that cannot be removed surgically due to their location or size. Sometimes radiation is supplemented with courses of chemotherapy.
- After surgical treatment. This type of radiation therapy is called adjuvant and is sometimes combined with chemotherapy. Radiation after surgery helps destroy remaining cancer cells and prevent recurrence.
- For advanced cancer. In this case, radiation therapy is aimed at combating pain, difficulty swallowing, bleeding and other symptoms.
Radiation is typically given five days a week for 6–7 weeks. If radiation therapy is used for palliative purposes, the course will be shorter.
Chemotherapy
Chemotherapy is used quite rarely for malignant neoplasms of the salivary glands. Anticancer drugs can reduce the size of the tumor, but are not able to completely destroy it. They are most often prescribed for advanced cancer as palliative treatment or in addition to radiation therapy.
Depending on the type and other characteristics of the cancer, the doctor may prescribe combinations of different chemotherapy drugs: carboplatin, cisplatin, 4-fluorouracil, doxorubicin, paclitaxel, cyclophosphamide, vinorelbine, docetaxel, methotrexate. Chemotherapy for cancer is always given in cycles. The patient is administered the drug, then takes a “break” for several days. The course of treatment may consist of several cycles.
Rehabilitation
After treatment, some problems associated with nerve damage may persist: dysfunction of the facial muscles, speech disorders, swallowing, and cosmetic defects. Some side effects of chemotherapy and radiation therapy go away after treatment is completed, while others persist for a long time. In such cases, rehabilitation courses are indicated. The doctor draws up a rehabilitation treatment program individually, depending on the severity and nature of the disorders.
Stages of the disease
Salivary gland cancer, like other malignant tumors, is classified into stages according to the generally accepted TNM system. The letter T in the abbreviation denotes the characteristics of the primary tumor: the size and degree of its growth into surrounding tissues, N - spread to the lymph nodes, M - the presence of distant metastases. Depending on these indicators, the following stages are distinguished during salivary gland cancer:
- Stage 0 is “cancer in situ” (carcinoma in situ). The tumor is located within the layer of cells that form the salivary gland and does not grow into neighboring tissues.
- Stage I is a tumor that is located within the salivary gland and measures no more than 2 cm.
- Stage II - the tumor reaches a size of more than 2 cm, but not more than 4 cm.
- Stage III - a tumor that reaches a size of more than 4 cm and/or spreads into surrounding tissues, or a tumor of any size that has grown into surrounding tissues, has spread to one cervical lymph node on the same side, and the focus in the lymph node is no more than 3 cm and does not extend beyond its borders.
- Stage IV includes substages IVA, IVB or IVC. The first two are characterized by varying degrees of spread of the malignant tumor to the anatomical structures of the head, neck, and lymph nodes. If stage IVC is diagnosed, it means that there are distant metastases.
In addition to stages, there are three degrees of malignancy of salivary gland cancer:
- Grade I - low degree of malignancy. Such tumors are called highly differentiated. Tumor tissue is as similar as possible to normal salivary gland tissue. It grows slowly, and the prognosis for such patients is most favorable.
- Grade II are moderately differentiated tumors. Tumor tissue differs more significantly from normal tissue. This cancer is more aggressive and has a poorer prognosis.
- III degree - poorly differentiated tumors. Cancer cells almost completely lose the features of normal ones. Such tumors behave the most aggressively.
Determining the degree of malignancy helps the doctor predict how the cancer will behave and plan treatment correctly.
Symptoms of the disease
Benign and malignant tumors of the salivary glands present with similar symptoms. One of the main differences is that cancer grows much faster and more often leads to a number of symptoms associated with growth into surrounding tissues and compression of nerves.
You need to visit a doctor if you are bothered by the following symptoms:
- A lump or swelling has appeared in the mouth, cheek, jaw, or neck.
- You have noticed that your face has become asymmetrical.
- I am worried about pain in the mouth, neck, ear, cheek, jaw. It doesn't last long.
- Numbness of part of the face.
- Weakness in the facial muscles, because of this, half of the face may be “lowered,” which becomes especially noticeable when baring teeth or frowning.
- I can't open my mouth wide.
- Difficulty swallowing.