When carrying out certain dental procedures, it may be necessary to reliably isolate the teeth from saliva, as well as the gums from the effects of chemicals used in treatment. For example, this is necessary when filling canals, restoring teeth and performing other complex procedures. Typically, special cotton or gauze swabs are used for these purposes. However, there is also such an alternative solution in dentistry as a rubber dam - a device that isolates the working surface from the mucous membrane during the treatment process.
Advantages and disadvantages of rubber dam
In dentistry, a rubber dam is a special rubber curtain that is installed on a tooth using clamps and isolates it from the surrounding oral cavity. This device is characterized by a whole list of indisputable advantages, among which the following are worth highlighting:
- reliable protection of the mucous membrane from the effects of chemicals;
- providing a good overview of the elements of the dentition;
- the ability to swallow during dental procedures;
- prevention of dry mouth;
- ensuring the most comfortable position of the tongue;
- eliminating the need to constantly change gauze swabs and rinse your mouth.
The use of rubber dam in dentistry significantly increases the degree of patient comfort during dental treatment. A person can breathe freely and swallow saliva, and the manifestations of the gag reflex are minimized. Patients note a decrease in fatigue of the masticatory muscles, which are usually in a tense state throughout the entire treatment process due to the need to keep the mouth open for a long time.
However, along with numerous advantages, the device in question also has a number of disadvantages, among which it is worth paying attention to:
- the possibility of developing an allergic reaction (silicone plates may be an alternative);
- possibility of injury to interdental papillae;
- the risk of losing axial landmarks when opening the entrance to the dental cavity;
- excessive requirements when conducting radiographic examinations.
If you have a problem similar to that described in this article, be sure to contact our specialists. Don't diagnose yourself!
Why you should call us now:
- We will answer all your questions in 3 minutes
- Free consultation
- The average work experience of doctors is 12 years
- Convenient location of clinics
Single contact phone number: +7
Make an appointment
Effective isolation of the working field
Such a dental device as a rubber dam has been known for quite a long time. In 1861, the GoodYear Company invented the vulcanization process. Just three years later, this technology found its way into dentistry: a certain Dr. Barnum came up with the idea of using a rubber scarf to isolate teeth during treatment. This moment can be considered the “birthday” of the rubber dam.
The use of a rubber dam has numerous advantages: it guarantees isolation from microorganisms, protects the patient from aspiration of instruments and detritus, and from contact with the mucous membrane of aggressive solutions and materials, and also protects the doctor from microorganisms and unpleasant odor from the patient’s mouth.
The following are counterarguments to the use of rubber dam:
- difficulty breathing for the patient;
- restriction of the patient's freedom of movement;
- inconvenience of applying the entire structure;
- the need to use hard steel clasps, which injure the hard tissues of the tooth.
There are many techniques for applying a rubber dam, and this often confuses doctors. The most common are two main methods.
According to the first of them, the selected clasp is fixed on the most distal tooth, after which the scarf, with the help of an assistant, is pulled first onto the clasp and then onto the frame.
The second method of applying a rubber dam is to make a hole in the latex scarf using a hole punch and then fix it on the frame. Subsequently, the required clasp is inserted into the hole in the scarf and the entire structure is applied to the most distally located tooth of those to be treated (Fig. 1).
Rice. 1
This method of applying a rubber dam is simpler and more common due to the fact that only a doctor works in the oral cavity (without an assistant). However, despite all the advantages of the above method, various difficulties and errors in application necessitated further optimization. This is how Kerr's OptiDam™ system was born and offers significant benefits.
First of all, the unusual three-dimensional design of OptiDam™ attracts attention. The idea of creating a 3D scarf for a rubber dam is driven by the need to reduce the pre-tension of the system.
This means that, in theory, OptiDam™ can be used without molar clasps, since the latex scarf lies passively in the mouth. While excessive tension on the scarf requires a rigid clasp to securely fix it, the absence of such tension allows one to avoid injury to hard and soft tissues.
The asymmetrical 3D shape of OptiDam™ Posterior (for posterior teeth) is no coincidence. The space in the area of the teeth to be treated is increased, which prevents accidental movement of the scarf due to unintentional movements of the doctor or patient (Fig. 2).
Rice. 2
In addition, sufficient space is also required for saliva removal by an assistant or a passively inserted saliva ejector into the oral cavity (Fig. 3), so the OptiDam™ does not take up too much space in the oral cavity on the side opposite to the intervention. At the same time, the scarf opens the corners of the patient’s lips, facilitating oral breathing.
Rice. 3
All these benefits are achieved not only due to the three-dimensional design of the scarf, but also thanks to the adjustable frame. The OptiDam™ frame is designed in such a way that its outline follows the lines of the lips when the mouth is open, its oval shape provides freedom of movement for the doctor and makes treatment more comfortable for the patient (Fig. 4).
Rice. 4
In addition, in the sagittal plane, the 3D contours of the frame also follow the contours of the face.
In the nose area, the rubber dam frame has a concave section, which facilitates nasal breathing for the patient. The pointed protrusions designed to secure the scarf in the OptiDam™ system are moved to special recesses on the frame, which eliminates the possibility of accidental injury. During treatment, this lip design makes it easier to collect various liquids that would normally splash onto the patient due to careless movements.
OptiDam™ Anterior (for the anterior group of teeth) has a symmetrical shape, as this is necessary to eliminate excess tension in the premolar area, in addition, it allows patients to move the lips away from the working field, and also ensures optimal aesthetics of restorations (Fig. 5).
Rice. 5
Thanks to the presence of special “papillae” on the surface of OptiDam™, located in the right place and having the right dimensions, the procedure for making holes in the rubber dam scarf becomes simple and predictable: in order to make a hole in the scarf, you simply need to cut off the top of the “papilla” using sharp scissors . The remaining uncut edges of the papilla face the gum and, when a rubber dam is applied, are immersed in the dental-gingival sulcus.
The depth of immersion depends on the height at which the top of the “papilla” was cut off. The advantages are easy gum retraction and the formation of a valve zone around the neck of the tooth, which is especially important in the anterior region, as it facilitates further modeling of the restoration.
Often, an objective determination of the color of the teeth becomes impossible after the application of a rubber dam due to their drying, however, the blue color of the scarf contributes to a more differentiated assessment of color, and also has a relaxing effect for the doctor’s eyes and increases the contrast of perception (Fig. 6).
Rice. 6
The application procedure for OptiDam™ Anterior is very simple. After making a hole of the required size, the scarf is put on a frame and usually fixed on the teeth symmetrically on opposite sides. The correct distance between the holes, as well as the sliding effect in a humid environment, facilitate the process of positioning the interdental septa of the scarf using floss (Fig. 7).
Rice. 7
To fix a rubber dam in the premolar area, a clasp is not always required: tying it with floss or using other auxiliary materials can solve this problem (Fig. 5). To immerse the edges of the scarf, located around the holes made, into the gingival sulcus, you can use an air gun (puster).
In difficult clinical situations, such as non-standard tooth position or the presence of a tooth defect below the gum level, the so-called adhesive technique is used. In these cases, the papillae on the scarf are not cut off, but with the help of scissors a long narrow incision is made along the dentition. Using tissue adhesive (Histoacryl®), the rubber dam is glued to the gum tissue on the vestibular and oral sides (Fig. 8).
Rice. 8
Once treatment is completed, the rubber dam is removed from the mouth without causing any damage to the soft tissue. In order to make the above incision in the correct place, the papillae on the scarf are used as a guide (Fig. 9): to ensure a tight fit of the rubber dam to the gum, the incision is placed along the buccal surface of the papillae. Thus, the possibilities of using a rubber dam are not limited to the placement of individual fillings, but also extend to more complex restoration techniques.
Rice. 9
“Upper” and “Lower” modifications of OptiDam™ Anterior are available with different papilla locations for the upper and lower dentition, which allows you to simultaneously apply a rubber dam to the anterior teeth of both jaws. This procedure was practically impossible with a conventional dental dam, so we can say that the OptiDam™ system opens up new possibilities, especially in the field of professional teeth whitening, since when using products with a peroxide content of up to 40%, complete isolation of the gums is a necessary condition. In addition, thanks to the concave edges of the holes in the scarf, the OptiDam™ system allows you to isolate a greater height of the clinical crown of the tooth (compared to traditional systems), which until now seemed impossible.
The use of OptiDam™ Posterior (for posterior teeth) does not differ significantly from traditional techniques, but it is significantly simplified due to the advantages described above (Fig. 10).
Rice. 10
If a clasp is used, we recommend (as when using any type of rubber dam) to pre-stretch the hole made in the scarf for passive insertion of the clasp. The range of possibilities is not limited to single restorations and includes more complex treatment techniques, such as adhesive fixation of metal-free prosthetics (Fig. 11).
Rice. eleven
The patient's comfort-oriented design and simplified application method make the rubber dam application procedure more enjoyable and safe even for an experienced specialist, and allow the novice to avoid the most common difficulties.
Adverse reactions
Dentistry uses a rubber dam made of rubber, which can cause an allergic reaction in some patients. In some cases, the cause of a negative reaction in the body may be talc, which is sprinkled on the preparatory plates. For example, some manufacturers produce options without the use of talc. A rubber dam is a type of dental device in question that is made from silicone. This material is characterized by many advantages, but has a weaker degree of elasticity.
Before introducing this technique into your dental practice, a specialist must master the technology of applying insulating protection itself. Incorrect use of this coating, as well as an error in selecting the thickness of the rubber pads, can lead to serious injury to the interdental papillae. The use of rubber dam in dentistry during the treatment process guarantees a long service life of the restored elements of the dentition.
The dental clinic “32 Dent” carries out all types of diagnostics and treatment of diseases of the teeth and oral cavity using the latest technologies, modern equipment and the best materials. To receive advice on all questions of interest, contact us by phone listed on the company’s website.
Isolation of one tooth
Minimally invasive preparation of 2.5 teeth for an all-ceramic crown
Initial situation: inadequate and unaesthetic restoration of tooth 2.5, failed obturation of the root canals (Fig. 2 a).
Repeated endodontic treatment: installation of rubber dam, creation of access; cleaning root canals from zinc-eugenol paste; filling the root canals of 2.5 teeth using the vertical condensation technique of hot gutta-percha (Fig. 2 b-e).
Rice. 2a. initial situation
Rice. 2b. Paste in channels
Rice. 2c. Working Rg with tools in channels
Rice. 2g. Canal mouths after paste removal
Rice. 2d. Control of root canal filling of 2.5 teeth
The effectiveness of antibiotics and folk remedies
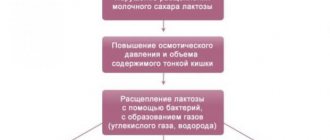
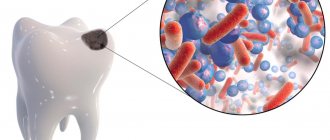
Pulpitis is a complication of carious processes that occurs as a result of infectious agents entering the tooth pulp. Caries is an irreversible process that can only be treated by drilling out rotten tissue. Experiments indicate that the microflora that causes caries is highly resistant to any antibiotics. For example, resistance to ampicillin is 99.99%, and to lincomycin - 95%. If bacteria have such a high resistance to antibiotics, then the use of “miracle” herbs and rinses is not even worth talking about.
Clinical picture
The intensity of pain in this disease can be very different: insignificant, arising as a result of exposure to thermal factors, and acute paroxysmal, causing genuine horror in the patient. Treatment of tooth pulpitis depends on clear symptoms. The severity of pain divides the disease into two conventional categories.
Acute form
This form is characterized by intense, acute and paroxysmal pain, intensifying at night. If you ignore the disease, pain increases, and pain-free periods shorten. Often pain appears on its own, even without the action of irritating factors. During the period of absence of pain, discomfort may arise due to exposure to thermal factors, for example, cool or hot food. The pain remains for another 10-15 minutes after the irritating factor has been eliminated (this characteristic helps differentiate inflammation of the neurovascular bundles of the tooth from carious processes).
In the case of caries, the pain recedes along with the irritating factor. Often, the patient is unable to accurately point to the tooth that hurts, since pain impulses seep through all the nerve trunks. Due to the smooth transition of serous inflammation to purulent inflammation, pain also increases. During the progression of purulent inflammatory processes, the pain becomes constant: there are no painless intervals.
Chronic form
In this case, the inflammatory process is not expressed. Often a person feels a slight aching pain in the teeth, which most often appears due to the action of cold and hot food. Sometimes there is no pain at all. This form of the disease can develop into an acute form: at this time the pain becomes especially pronounced.
Bridge insulation: superfloss
Treatment of pulpitis of the 2.1 tooth, which is the support of a bridge prosthesis
Initial situation: pulpitis of the central incisor, previously restored with a metal-ceramic crown, was diagnosed (Fig. 4 a, b).
| Rice. 4 a, b. Initial radiograph 2.1 |
The problem of placing a rubber dam on a bridge can be overcome by tying the connecting elements with superfloss.
Endodontic treatment: traversing, cleaning and shaping the root canal; filling the canal using the method of vertical condensation of hot gutta-percha; composite restoration of the palatal surface (Fig. 4 c-f).
Rice. 4c. Working Rg with gutta-percha cone in the canal
Rice. 4g. Shape of the root canal mouth
Rice. 4d. Restoration of the palatal surface
Rice. 4e. Control radiograph