Traumatologist-orthopedist
Shelepov
Alexander Sergeevich
13 years of experience
Doctor
Make an appointment
Many people mistake a small bulge that appears on the bone as the result of an injury. Education in the early stages does not create any special problems or cause discomfort, so a visit to the doctor is postponed. As a result, patients consult a doctor after the onset of painful sensations, when the osteoma becomes visually noticeable, begins to cause severe discomfort and leads to deterioration of health.
Osteoma is a benign tumor-like neoplasm developing from bone tissue, which is not predisposed to transition to a malignant state. It develops slowly. Osteoma is dangerous because it develops imperceptibly, without pronounced symptoms, so most people turn to doctors when the pathology is severely advanced and long-term treatment is necessary. Osteoma grows slowly, which allows patients to be successfully treated if treated in a timely manner.
Types of osteomas
Diagnosis of osteoma involves differentiation from similar neoplasms and determination of its type in order to select subsequent treatment.
Tumors are divided by number, type of tissue they are made of, method of germination and complexity of structure. Each of them can be located in different parts of the musculoskeletal system and provoke different symptoms. Based on the number of tumors, they are divided into single (solitary) and multiple, and based on their composition into solid, spongy and medullary. The first consist entirely of bone tissue without bone marrow, the second of spongy substance, and the third of bone marrow cavities. Tumors originate from different tissues (bone or connective) and because of this they have different names:
- hyperplastic – consist exclusively of bone (osteomas and osteoid osteomas),
- heteroplastic - osteophytes, composed of different tissues.
Osteomas are composed of normal bone tissue, are localized on the bones of the skull, and often put pressure on neighboring organs, such as the eyes. Osteoid osteomas consist of osteogenic tissue penetrated by blood vessels, bone membranes, areas of destroyed bone tissue, and are localized anywhere, in 50% of cases - on the tibia. At the initial stage of development of the disease, there are no symptoms, and then a flat, thin infiltrate appears (if we talk about epiphyseal osteoma, it accumulates in the joint). If in children this type of tumor occurs in the bone growth zone, then one limb will increase in length.
Osteophytes are also divided into 2 types - ectostoses, which grow from above (the skull, face, pelvic bones are the favorite places for their localization), and enostoses, internal, growing into the medullary canal. Exostoses have the shape of a hemisphere, cauliflower, thorn, or mushroom. One of the features of osteophytes (heteroplastic osteomas) is that they appear on the diaphragm, lining of the heart, brain tissue, etc.
Causes of osteoma of the jaw
To this day, experts cannot make a final conclusion about why a particular person developed osteoma. The medical research they carried out only allowed them to identify a number of provoking factors that can cause a failure in the division of bone cells - it is from them that a pathological focus in the jaw is subsequently formed.
Most often, a relationship is established with the following negative factors:
- suffered maxillofacial injuries, even without fracture of bone structures;
- various chronic inflammatory processes - for example, osteomyelitis, sinusitis, dental caries;
- poor-quality dental procedures performed - particles of material remain in the sinuses;
- X-ray and other imaging diagnostic procedures performed too frequently;
- exposure to ionizing radiation – for example, radiation therapy for skull tumors.
Less often, oncologists come to the conclusion that the formation of osteoma is based on a person’s harmful individual habits – abuse of tobacco and alcohol products. In some cases, it is not possible to draw a conclusion about what was the root cause of the development of the disease.
Causes
The cause of osteoma is said to be heredity, but its appearance and progression can also be facilitated by certain diseases, including gout, syphilis and rheumatism (the trigger is often trauma, especially repeated trauma). The pathology of calcium metabolism sometimes causes the development of inert tumors, the pathological development of embryonic cells can lead to the development of growths, and when localized in the nasal sinuses - a purulent complication or inflammation, puncture of the maxillary sinus. Ectostoses can form during puberty.
Factors
There is a consensus among experts on the question “what are the reasons for the formation of such a tumor?” does not exist. It is argued that there is a connection between osteoma of the jaw and a number of factors. These include:
- Trauma to the maxillofacial bones, chronic or one-time (bruise, damage to the integrity of the oral mucosa, untreated teeth (which caused them to quickly collapse), tartar (hard dental deposits), dentures and dental implant crowns that change the bite (poorly fitted) ), poor surface treatment of dental fillings that do not allow the jaws to fully close).
- Inflammation in the area of the nose and jaw (actinomycosis, sinusitis, periodontitis, osteomyelitis, periostitis, sinusitis and other pathologies), chronic or acute.
- Aggressive environmental effects (smoking, chemical, ionizing and radioactive exposure).
- Foreign particles in the sinuses above the upper jaw (often fragments of teeth or particles of materials used to fill teeth).
Experts do not classify osteoma itself as an odontogenic disease. But there are factors that provoke the appearance of a tumor.
Symptoms
The signs of osteomas depend on the location, are not similar to each other, and are sometimes difficult to differentiate due to symptoms similar to other common diseases. It is easier to make a diagnosis in the presence of convex external tumors that are visible to the naked eye.
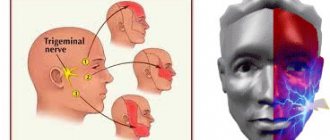
If the tumor is located on the bones of the head, depending on the location, symptoms are observed:
- on the posterior wall of the frontal sinus - intracranial pressure, headaches (do not go away), size from 2 to 30 mm;
- on the lower wall of the frontal sinus - moving the eye forward;
- on the frontal bone (internal plates) - memory problems, headaches, seizures with convulsions, intracranial pressure;
- in the nasal cavity - difficulty breathing through the nose, decreased sense of smell, problems with the eyes (drooping eyelid, double vision, decreased vision);
- on the occipital bone - pain in the head, sometimes epileptic seizures;
- on the parietal and temporal bone - noticeable, but does not cause painful symptoms;
- on the lower jaw (lateral branch or posterior side) - when compressing the soft tissues of the muscles, they can lead to asymmetry and dysfunction, the edges of the tumor are smooth, and the shape is oval or round.
In addition to the bones of the skull, the tumor also affects the bones of other parts of the musculoskeletal system, respectively, symptoms of osteoma and pain appear at its location:
- thigh bones - muscle pain, worse at night, swelling in the legs, altered gait;
- knee joint - makes movement difficult;
- vertebral arch or its process – the formation of scoliosis, symptoms of spinal compression, pain.
Pain due to osteophytes is eliminated completely or partially with the help of analgesics, however, if there are regular repeated attacks of pain, difficulty moving, or the appearance of visible lumps, you should immediately consult a doctor to avoid complications.
Diagnostics
Diagnosis of the tumor is carried out to determine its type and location in order to select tactics for treating osteoma. As part of its implementation, X-ray and CT are used. The most informative is a 3D reconstruction; it shows all the details and outlines, as well as the extent of damage to surrounding tissues. In the process, it is important to differentiate osteoma from chronic Brody’s abscess, organized periosteal callus, osteochondrosis dissecans, osteogenic sarcoma, osteoperiostitis and other diseases.
Before prescribing an x-ray or tomography, the doctor conducts an examination and identifies:
- presence of pain when pressing;
- location;
- growth rate;
- functionality of the tissue that has been affected.
Using X-rays, a specialist detects the number of tumors, their structure, location, and the degree of bone destruction. It should be noted that on an x-ray the exostosis looks smaller than in reality, since its upper cartilaginous layer is not visible. In children it reaches a thickness of several centimeters. The benign nature of the tumor is indicated by correct geometry and structure, a clear contour, a small degree of calcification and growth at a low rate.
Treatment
Removal of osteoma is indicated if it compresses neighboring organs, is visible visually, that is, acts as a cosmetic defect (especially on the face and head), changes the shape of bones, reduces mobility, leads to scoliosis, and causes pain. Most often, tumors are removed from the sinuses, ear canal, jaws, knee and hip joints.
If the tumor does not manifest itself in any way and does not cause discomfort, the doctor observes it and evaluates its growth rate. A small osteoma that has stopped growing does not need to be removed or treated.
The operation to remove the tumor is performed by maxillofacial surgeons or neurosurgeons. During the operation, the doctor cuts the tissue, removes the growth and part of the bone/tissue around it to avoid relapse.
The doctor will suggest removing the osteoma in the following ways:
- complete excision – used for tumors in the sphenoid sinus;
- curettage - an incision in the skin, removal of a tumor, cleansing the lesion by curettage;
- endoscopic removal - suitable for small tumors with a difficult approach, used using computed tomography to monitor the progress of the operation and a radiofrequency probe, takes about 2 hours.
Tumor recurrence occurs in 10% of cases due to incomplete removal. To exclude this possibility, you need to choose a good clinic and specialist.
Services and prices
Mandibular cancer is a primary or secondary (metastatic) malignant tumor affecting the mandibular bone.
Diagnosis of cancer of the lower jaw includes collecting complaints, taking a history of the disease, physical examination, and radiography.
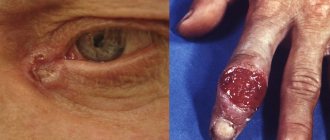
The results of a cytological examination are decisive in making a diagnosis. In case of secondary cancer of the lower jaw, a crater-shaped ulcerative surface with a dense bottom covered with a gray coating and ragged, corroded infiltrated edges is revealed on the mucous membrane of the alveolar process in the area of the transition of the fixed mucosa to the mobile one. On palpation, pain and bleeding are noted.
Cancer of the lower jaw is a malignant neoplasm characterized by an infiltrative type of growth and early metastasis. Patients indicate the appearance of acute paroxysmal pain radiating along the mandibular nerve, paresthesia of the lower lip and mental area, and the presence of pathological mobility of intact teeth. Diagnosis of cancer of the lower jaw includes clinical, radiological and cytological studies. Treatment of cancer of the lower jaw consists of pre- and postoperative telegammatherapy, radical resection of the affected part of the bone. If metastases are detected, lymphadenectomy is performed.
Cancer of the lower jaw is diagnosed less frequently than that of the upper jaw. For one case of cancer of the lower jaw, there is one case of sarcoma of the same location. The primary tumor process is detected mainly in men after 40-45 years of age. More often, a malignant neoplasm is localized in the molar area. Metastatic cancer of the lower jaw occurs mainly in women due to metastasis of tumors of the breast and stomach. Histogenetically, cancer of the lower jaw in the vast majority of cases is squamous cell keratinizing.
Causes of cancer of the lower jaw
The main causes of cancer of the lower jaw are obligate and facultative precancers of the mucous membrane lining the alveolar process. A malignant lesion of bone tissue develops as a result of malignancy of papillomatosis, erosive or verrucous form of leukoplakia. With a long-term decubital ulcer of the mucous membrane, which appears as a result of chronic trauma from the sharp edges of destroyed teeth, the risks of the inflammatory process transitioning into a tumor are also high.
Cancer of the lower jaw can also occur as a result of the growth of a malignant neoplasm into the bone from adjacent anatomical areas. Tumor cells can spread to bone tissue from the floor of the mouth, the retromolar area. In rare cases, patients with primary cancer of the lower jaw, which develops directly in the bone from the remains of a tooth germ or epithelial cells of the lining of an odontogenic cyst, turn to dentistry.
Classification and symptoms of cancer of the lower jaw
Based on the prevalence of the tumor, the following stages of cancer of the lower jaw are distinguished:
- T1 – malignant neoplasm is localized within one anatomical region.
- T2 – cancer of the lower jaw has spread to two adjacent areas.
- T3 – the tumor extends beyond two anatomical regions.
- T4 – the entire organ is involved in the tumor process.
Diagnosis of cancer of the lower jaw
Diagnosis of cancer of the lower jaw includes collecting complaints, taking a history of the disease, physical examination, and radiography. The results of a cytological examination are decisive in making a diagnosis. In case of secondary cancer of the lower jaw, a crater-shaped ulcerative surface with a dense bottom covered with a gray coating and ragged, corroded infiltrated edges is revealed on the mucous membrane of the alveolar process in the area of the transition of the fixed mucosa to the mobile one. On palpation, pain and bleeding are noted.
For a cytological examination, the dentist takes a scraping from the ulcer surface. In case of central cancer, it is impossible to take material for research by puncture due to the high density of the bone tissue of the lower jaw. In this case, bone trepanation is indicated. If enlarged lymph nodes are detected, they are punctured, followed by a cytological examination of the contents. To diagnose cancer of the lower jaw, a radioisotope method is also used, which is based on the ability of a malignant neoplasm to accumulate the p32 isotope.
Treatment of cancer of the lower jaw
Cancer of the lower jaw requires combined treatment. At the preoperative stage, a number of orthopedic measures are performed (taking impressions, making structures to fix the remaining part of the jaw in the previous position). Mobile teeth are not removed due to the high risk of lymphogenous dissemination of cancer cells. This is followed by a course of gamma therapy, after which surgery is performed 3 weeks later. For superficial lesions of the alveolar process, a through resection is performed, retreating on both sides of the pathological focus.
If the cancer of the lower jaw is localized in the middle of the lateral region, a section of bone is removed from the mental region to the mandibular foramen. If the angular zone is involved in the tumor process, resection of half of the mandibular bone begins. If the chin is affected, the mandibular bone must be removed from corner to corner. In the case of metastasis of mandibular cancer to regional lymph nodes, radical excision of the lymphatic system along with the subcutaneous tissue, accessory nerve, sternocleidomastoid muscle, and submandibular gland is indicated.
When cancer of the lower jaw spreads to the tongue, palate, parotid salivary gland and pharynx, all tissue affected by the tumor process must be removed. Gamma therapy is also carried out in the postoperative period. Reconstructive surgeries aimed at replacing bone defects are recommended to be performed no earlier than one year after surgery. If an inoperable malignant tumor is diagnosed, a course of palliative radiation therapy is prescribed. Squamous cell keratinizing carcinoma cells are insensitive to chemotherapy.
Is osteoma dangerous?
Speaking about the dangers of osteoma, one should note first of all the compression of neighboring organs and symptoms that cause inconvenience to the patient. If the tumor does not manifest itself and does not grow, it can be left in place. A neoplasm of this kind never develops into malignant – there is no need to be afraid of cancer. Tumors on the head should be treated with particular care - they not only cause unpleasant symptoms, but can also lead to a brain abscess. As a rule, they are removed surgically.
Etiology and pathogenesis
The causes and origin of osteoma are not fully known. Some researchers consider it a neoplasm that develops at a certain time. Others tend to classify the lesion as an anomaly of the craniofacial bones.
Doctors also named the following as possible etiological factors:
- trauma, since most formations are located in the lower part, which is more susceptible to traumatic lesions;
- combination of injury and muscle strain;
- infectious or inflammatory processes of the oral cavity or jaw bone tissue
Study of the etiology of benign jaw lesions