Modern dentistry allows not only to treat oral diseases, but also to improve the aesthetic appearance of teeth. In other words, make your smile beautiful. The Denta-Professional clinic offers a wide range of aesthetic dentistry services.
We use only modern working methods, high-quality certified materials, and our offices are equipped with the latest equipment. Over our 21 years of existence, we have helped thousands of people gain a beautiful smile and self-confidence.
Aesthetic dentistry is a direction in dental practice, the task of which is to eliminate various defects in the appearance of teeth and dentition. According to modern beauty standards, the dentition should be smooth, and the dental units themselves should be a natural white color, with microrelief and a transparent cutting edge.
Types of aesthetic dentistry
Depending on the aesthetic task, approaches to work may be different. If a complete change in the appearance of the entire dentition is required, then usually one procedure cannot get rid of it. Complex work of several specialists will be required: gnathologist, orthodontist, surgeon and orthopedist.
If we are talking about less global changes, for example, the restoration of one or more destroyed units, chipped front teeth or changing the appearance of the smile area, the following procedures may be used:
- Restoration with composite materials
- Restoration of chewing teeth with inlays
- Aesthetic (artistic) restoration of anterior teeth
- Aesthetic restoration with veneers
Teeth whitening also falls within the scope of aesthetic dentistry.
The most effective methods
To restore the appearance of the unit you need to:
- after injuries;
- in the presence of congenital aesthetic defects;
- after certain types of dental treatment.
This procedure is used as an alternative to enamel whitening for the visual correction of malocclusions. There are many ways to perform artistic dental restoration. Prices, materials, treatment methods may vary. But dentists consider three methods to be the most effective and safe:
- veneers;
- lumineers;
- tabs.
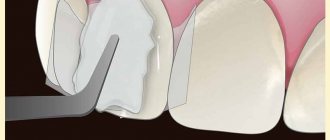
Veneers are thin, from 0.2 mm, plates. They are attached to the outer surface of the units. Aesthetic restoration of teeth with composite or porcelain is possible. Veneers are also used for other purposes. These plates protect the enamel from mechanical stress. For example, they are recommended to be installed by musicians who play wind instruments. Typically the unit will need to be ground down a bit to install the plates. If this is not done, it will turn out to be thicker than its neighbors and will stand out from the series. But there are situations when veneers are attached directly to the enamel - for example, if the unit was initially erased.
Lumineers are also plates, but ultra-thin. They are made from ceramics using a special technology patented by the American company Cerinate. The procedure is non-traumatic - there is no need to grind down the enamel. An inlay is a “hybrid” of a crown and a filling. It replaces the missing part of the unit. It can be metal, ceramic, metal-ceramic or composite. Ceramic inlays are indistinguishable from enamel either in color or transparency.
Restoration with composite materials
To restore the coronal part, dentists use composite light-curing materials, the same ones used for fillings. This procedure is usually used when a tooth with minor damage needs to be restored. The composite material is quite fragile and will not be able to fully restore functionality on chewing teeth if the chip is large.
The service life of such a restoration is individual for each patient and depends on the structural features of his teeth and physiological properties. Bad habits and oral care also have a big impact. The average lifespan of a light seal is 5 years, but it often lasts much longer.
Reviews from our patients
I really liked it, EVERYTHING was great!
Good attitude and professionalism of doctors! Tikhomirov E.V.
She underwent a course of treatment at the Laser Dentistry Clinic. Now I have a radiant smile and am always in a good mood. You just have golden hands. For the first time I felt what treatment was like without pain. High professionalism plus attentive attitude towards people are the distinctive features of the clinic. Thank you again for the opportunity to go through life with a smile and wish you success in all your endeavors!
Casanova O.I
Artistic restoration of anterior teeth using composite materials
The same procedure as conventional restoration, but performed in the visible area of the smile. It requires the dentist to work much more carefully on the appearance. If in the case of restoration of a chewing tooth one color and material are used, then when it is necessary to remove a chip on the front tooth, the dentist must repeat the adjacent dental units in detail so that the restored tooth does not stand out.
The natural appearance of dental units is partial transparency, heterogeneity and microrelief. This effect can only be achieved using materials of several colors. When performing this procedure, the therapist, like a sculptor, restores the tooth, layer by layer applying different materials. Therefore, such restoration is called artistic.
Dental jewelry? It's fashionable
Part of aesthetic dentistry is not only giving teeth a natural look, but also decorating them. In particular, so-called skyes—dental jewelry—are now very popular. They are small precious or semi-precious stones that are glued to the surface of the tooth.
Installing skyes is quite safe and painless - the dentist sticks a small pebble onto the previously prepared tooth enamel using special glue. You can also order a skyce when installing a filling, during extensions - but in this case it will be more difficult to remove it.
Important: With such a small detail you can not only decorate a tooth, but also hide minor enamel imperfections, fillings or extensions. And, of course, skys look attractive and unusual - they emphasize a perfect smile and all the advantages of appearance.
All these services, which will make up your ideal smile, can be ordered from any of our clinics. Therefore, do not hesitate - choose the branch that suits you and come become more attractive.
Dental restoration with veneers
Veneers are thin shells that are glued to the tooth and can improve the aesthetic appeal of the dentition. Restoration with veneers is, in fact, prosthetics performed by an orthopedic dentist. Various types of veneers can be used for the procedure:
- from composite materials (therapeutic or composite materials)
- ceramic (orthopedic);
Veneers made of composite materials. These are plates made of a material similar to that from which fillings are made. Only in the case of veneers does production take place entirely in the factory. Already in the patient's mouth, each veneer is individually adjusted to the tooth. This can also be done by a general practitioner, which is why they are otherwise called therapeutic veneers. In our clinic we offer the best composite veneers from the Swiss company Colten.
Ceramic veneers . The best option for aesthetic restoration in the smile area. They are made in the laboratory individually for the patient’s teeth from durable ceramics. At the same time, they have the most natural appearance. Ready-made ceramic veneers look like “natural” teeth, so it is almost impossible to recognize them visually. Their service life is long - on average it is 20 years. Of course, ceramic veneers are more expensive than composite veneers. However, it is ceramics that provide ideal dental aesthetics and long-term results.
Aesthetics of anterior teeth. Successful planning
When restoring damaged or missing front teeth, esthetics is of paramount importance for most patients. At the same time, the achieved result must be durable. Using a clinical case as an example, this article discusses an effective concept for the manufacture of implant-supported anterior restorations. Important factors for successful treatment are 3D computer planning, transgingival placement of implants, osseointegration under the influence of functional loading and reducing any manipulation of the implants and surrounding hard and soft tissues to a minimum.
Introduction.
The front teeth are in line of sight. They have a very big impact on a person’s appearance and self-confidence. Therefore, when it comes to the restoration of anterior teeth, almost all patients become very critical and demanding. Already during the first consultation, the doctor must present to the patient all possible treatment options and be sure to note the advantages and disadvantages of each of them.
During the planning process, it is necessary to analyze the entire situation as a whole, as well as make the most reliable forecast of the patient’s general health and the state of his dental system. For lost front teeth, there are 3 possible treatment options: a removable denture, a tooth-supported bridge, and an implant-supported restoration. Removable restorations can only be considered as a temporary solution. The possibility of producing classic bridges supported by natural teeth should also be considered very critically, especially considering the longevity of implants, which have a survival rate of 93–96% after 12 years.
Covering teeth with crowns, even with optimal preparation, always causes additional stress on the periodontium, which significantly worsens the prognosis for the durability of bridges. From a biomechanical point of view, depending on the shape of the alveolar process of the upper jaw and the position of the teeth being restored, the manufacture of a canine-supported bridge is also quite problematic. In this case, the condition of the periodontium near the supporting teeth and the ratio of the working and balancing shoulder of force application are of great importance.
Under certain conditions, the first premolars are used as additional support for the bridge. In this case, the risks associated with covering teeth with crowns double. The survival rate of bridges, depending on the period of observation, ranges from 98% (5 years) to 28% (25 years). After 10 years, this value is 76%. There are a number of other reasons in favor of fabricating implant-supported restorations. If chewing teeth are lost, implants in the area of the front teeth can become the basis for a new restoration.
Even in the era of 3D and CAD/CAM, diagnostic models and 2D x-rays are used as input for planning. In some cases, for example, for installing implants in the area of chewing teeth with a sufficient amount of bone tissue, these materials may be quite sufficient for successful implantation. In more complex situations, it is very difficult to obtain all the necessary information using only these materials. In this situation, the most optimal and reliable option is to conduct three-dimensional diagnostics, for example, using digital volumetric tomography (DVT). However, one should not think that the use of DVT, computed tomography and navigation (Guided Surgery) alone guarantees success. Computer diagnostics and planning cannot replace a doctor, who must independently assess the real situation during a surgical operation and make the right decision. Even if it contradicts the computer's suggestions. Making the final decision and responsibility for it was and remains the prerogative of man.
Let's consider an example of restoration of anterior teeth using modern methods of diagnosis, planning and treatment.
Description of a clinical case. Initial situation.
A 50-year-old patient came in with a desire to improve the aesthetic characteristics of her smile. She wants to smile freely and not be shy about showing her teeth. During the clinical examination, the patient was found to have numerous fillings and generalized periodontitis of the upper jaw (Fig. 1). The incisors of the upper jaw have 3 degrees of mobility and are connected into a common block with composite material. Due to high mobility, combined with bone tissue atrophy at 2/3 of the height and poor condition of hard tissues, these teeth cannot be preserved. Therefore they were removed.
Rice. 1. Initial situation. In the anterior part of the upper jaw there is destruction of bone tissue and mobility of teeth of the 3rd degree.
Planning is the basis of success.
The patient was offered an implant-supported restoration. As part of a comprehensive sanitation of the oral cavity, it is planned to treat periodontal diseases. A temporary restoration is installed in place of the extracted teeth. Implantation planning is carried out several months after successful healing of the extraction alveoli and stabilization of the structure of the alveolar process of the upper jaw (Fig. 2).
Rice. 2. After 4 months, stabilization of the structure of the alveolar process of the upper jaw is observed. The initial conditions are favorable for the installation of implants. Depressions in the mucous membrane are formed using a temporary removable restoration.
Currently, the gold standard is the so-called Backward Planning, where the position of the implants is selected based on a model of the final result. At the first stage of planning, the teeth are set on a diagnostic model installed in the articulator (Fig. 3). Wax-up allows you to solve several problems at once, get an accurate idea of the planned treatment result, optimize the relative position of teeth and choose the optimal position of implants. In addition, a diagnostic template and a temporary bridge are made based on Wax-up (Fig. 4).
Rice. 3. The main element of Backward Planning is Wax-up. When modeling, it is necessary to take into account the expected load on the implants and orthopedic structure.
Rice. 4. A diagnostic template is made based on Wax-up.
If there is a deficiency of bone tissue and free space, implantation planning is best done using computed tomography or digital volumetric tomography. However, to assess the need for such a diagnosis, the panoramic x-ray and the diagnostic models in the articulator must first be analyzed. Volumetric images allow you to obtain and save all the information necessary to select the position of the implants in all 3 planes. The main task is to choose the optimal position in relation to the future restoration. On the other hand, it is necessary to take into account the quantity and quality of bone tissue in the planned position. Ultimately we must find a compromise between these two conditions.
The diagnostic template allows you to clearly transfer the position of the teeth being restored to DVT images (Fig. 5). During the planning process, we must always be clear about the desired end result - a high-quality restoration with impeccable aesthetic characteristics and a guarantee of durability. In this case, this means that to restore the natural shape of the gingival margin, the minimum thickness of the vestibular cortical plate must be 1 mm. The shape and structure of the papillae depends on the distance between the implants and adjacent teeth: it should be 1.5–2.0 mm. The design of the implants is of great importance. Ankylos implants (DENTSPLY Friadent) are placed subcrestally, making it much easier to create an optimal crown-to-soft tissue ratio using abutments or crowns. Experience shows that the less hard and soft tissues in the implantation area are injured, the better the prognosis for the longevity of the achieved results.
Rice. 5. DVT images provide the basis for implant position selection using ExpertEase (DENTSPLY Friadent).
During the planning process we must make the final choice of the implant system. For planned osseointegration under functional loads, implants whose macro- and microdesign ensure maximum primary stability are best suited. For this situation, the Ankylos C/X implant system (DENTSPLY Friadent) was chosen. At the same time, the diameter and length of each implant is selected.
The possibility of osseointegration under the influence of functional loads can only be assessed after determining the optimal position of the implants. In this case, this is possible, since the planning results are checked during the operation and indicate the presence of a sufficient amount of bone tissue. No additional augmentation is required. Under such conditions, the durability of implants whose osseointegration occurs under the influence of functional loads is at the same level as the durability of implants that are osseointegrated in a closed state.
An important factor for the success of the immediate loading concept is the high primary stability of the implants. The progressive thread design of Ankylos implants increases their primary stability even in difficult situations.
There are several other reasons why these particular implants are ideal for osseointegration under functional loads. The conical connection between implant and abutment ensures that there are no gaps. This reduces their micromobility and also prevents the penetration of bacteria, which is very important at the stage of healing of the surgical wound.
Installation of implants.
To transfer the planned position of the implants into the oral cavity, an appropriate surgical template must be made (Fig. 6). The ability to produce such templates is supported by all modern planning systems, for example ExpertEase (DENTSPLY Friadent). The planning results are sent to a specialized center and after 3-5 days the surgical template is ready. In this case, based on natural teeth.
Rice. 6. Based on the planning results, an appropriate surgical template is made. Fixing the template on natural teeth ensures its high stability and high accuracy of implant placement.
Any surgical intervention should be as gentle as possible. Minimally invasive involves minimal damage or injury to soft and hard tissues. In this case, this means that during the operation it is necessary to minimize damage to the vestibular cortical plate. The optimal solution to this problem is transgingival installation of implants in combination with careful preparation of the bone bed. Mobilization of large mucoperiosteal flaps when working in included dentition defects should be considered as an exception and not as a rule. The results of DVT together with palpation of the alveolar process allow us to obtain all the necessary topographic data for implant placement. The surgical template clearly sets the direction for the pilot bur. This means that there are no objective indications for preparing a mucoperiosteal flap.
Perforation of the mucous membrane.
Preserving the maximum amount of bone tissue in the implantation area, especially the cortical plate, is an important condition for ensuring the longevity of treatment results. Nutrition of cortical bone tissue is carried out through the periosteum. Preparation of a mucoperiosteal flap disrupts the blood supply to bone tissue for a long time, which can lead to their resorption. Perforation of the gums and periosteum only at the site of implant installation (flapless surgery) can largely solve this problem. In addition, transgingival installation of implants reduces pain and suffering of patients in the postoperative period.
After marking the puncture site, the mucous membrane is perforated (Fig. 7). The diameter of the hole should be approximately equal to the diameter of the implant. This operation can be carried out manually or using a special tool (Fig. 8). Soft tissue is removed from the hole with a scalpel and tweezers or a sharp spoon (Fig. 9).
Rice. 7. Designation of the site of transgingival implant installation on the surface of the mucous membrane.
Rice. 8. Perforation of soft tissues.
Rice. 9. A scalpel or sharp spoon is used to remove soft tissue from the hole. Transgingival installation of implants helps prevent resorption of surrounding bone tissue.
Preparation of the bone bed.
Sequential preparation of the bone bed is also carried out in accordance with the diameter of the selected implants (Fig. 10, 11). The surgical template specifies the position of each bur and the direction of preparation. The depth of preparation is constantly monitored (Fig. 11, 12). Depending on the quality of the bone tissue, the cortical part of the bed is modified with reamers (Fig. 13). For bone tissues D1 and D2, the development ensures optimal matching of the shape of the bone bed and the cortical part of the implants. This is an important condition for reducing trauma to bone tissue and ensuring the primary stability of implants.
Rice. 10. Preparation of the bone bed begins with a pilot bur.
Rice. 11. The primary hole is sequentially expanded in accordance with the diameter of the implant.
Rice. 12. If there is no limiter on the template or burs, then the preparation of the bed should be carried out with constant control of the depth.
Rice. 13. The use of a reamer ensures optimal matching of the shape of the bone bed and the cortical part of the implants.
Ankylos C/X implants are placed subcrestally. The structural features of these implants, the conical connection to the abutments, the surface roughness, as well as the Platform-Switching function, require the preservation of cortical bone tissue. The results of histological studies confirm that part of the bone tissue is located above the shoulder of the implant. This is another important condition for ensuring the stability of soft and hard tissues in the area of implantation and the durability of the achieved parameters of “red” and “white” aesthetics.
Installation of implants.
Implants can be installed manually or using a special key (Fig. 14, 15). The latter option is preferable, since in this case the implants are installed in the bone tissue with the same amount of torque. This protects the tissues from local overloads. The control image clearly shows that the implant is installed in exactly the planned position (Fig. 16).
Rice. 14, 15. In the final position, the implants are installed using a key. The indentations on the rotating tool are consistent with the indexes on the Ankylos C/X implants. In the final position, these elements should be on the vestibular surface.
Rice. 16. The result of precise implementation of all working steps is the identity of the planned and actual position of the implants.
The indentations on the rotating tool match the indicators on the Ankylos C/X implants (Fig. 14). In the final position, these elements should be on the vestibular surface. This is very important for subsequent work with indexed abutments. If you plan to work with non-indexed abutments, then the position of these elements does not matter. However, if there is a future possibility of replacing the external structure or extending the restoration, then it is much better to use indexed abutments.
Immediate fixation of the temporary restoration.
For osseointegration of implants under the influence of functional loads, it is necessary to make a temporary bridge. To minimize any manipulation of the implants, an impression is made using seating abutments (Figs. 17–19). A temporary bridge is made based on the original Wax-up (Fig. 20). In order not to make the patient wait, the prosthesis is made in advance. On the model cast on the basis of a new impression, the dental technician only connects it to the installation abutments (Fig. 20, 21). Correction of the base surface and occlusion surface is carried out directly in the oral cavity. During protrusion, the temporary denture should not come into contact with the anterior teeth of the lower jaw (Fig. 22). This prevents the impact of unfavorable loads on the implants during their osseointegration.
Rice. 17. To minimize any manipulation of the installed implants, a temporary bridge is made outside the mouth.
Rice. 18. Temporary sealing of the installation abutment channels.
Rice. 19. Cast for making a temporary restoration.
Rice. 20. A temporary bridge is made from the original Wax-up.
Rice. 21. The dental technician prepares a temporary restoration in advance and only fits it.
Rice. 22. Monitoring the accuracy of fixation of temporary restoration. During protrusion, it should not come into contact with the front teeth of the lower jaw.
Prosthetics.
Two types of abutments can be used with Ankylos C/X implants - indexed and non-indexed. Non-indexed abutments are marked “C/”. The implant is connected to the abutment only along a cone, which allows it to be installed in any position. Indexed abutments are marked “/X”. These abutments can be installed in one of 6 fixed positions. Despite the presence of an index, the stability of these abutments and anti-rotation protection is ensured by the conical connection. Both types of abutments can be freely adapted to the actual design or future modified restoration. From a clinical point of view, it is more convenient to work with indexed abutments, especially when several implants are connected by one framework. The presence of an index facilitates the installation of abutments in the same position on the model and in the oral cavity. Therefore, in this case we decided to use indexed abutments.
The production of permanent restoration begins 3 months after installation of the implants. In addition to the impact of functional loads, temporary restoration is used to form an optimal soft tissue structure (Fig. 23, 24). The photographs clearly show depressions in the soft tissues in the area of the central incisors. They help to camouflage the cervical areas of the bridge pontics and give them a natural appearance. Preparation and making of an impression using an individual tray are carried out using traditional technology (Fig. 23–26).
Rice. 23. After 3 months, the fabrication of the permanent restoration begins.
Rice. 24. Ankylos Regular /X transfer abutments (indexed) for making an in situ impression.
Rice. 25. To remove the impression from the oral cavity, it is necessary to remove the fixing screws.
Rice. 26. Before casting the model, implant analogues are installed in the impression.
In this case, the connection of the implants to the tertiary framework is carried out using Ankylos Regular /X abutments (Fig. 27). The groove-shaped shoulder and inclination angle of standard abutments are adjusted individually. The relationship between crowns and soft tissues is formed at the level of the abutments (Fig. 28). The tertiary frame is cast from a high gold content alloy. If desired, the tertiary framework can be manufactured using CAD/CAM techniques from another alloy or zirconia. The latter is most appropriate for patients with thin gum biotype.
Rice. 27. Ankylos Regular/X abutment.
Rice. 28. The relationship between crowns and soft tissues is formed at the level of the abutments.
Fitting and cladding of the frame.
Trying on the frame allows us to evaluate the quality of all previously completed work stages. A polymer template is pre-made, which greatly facilitates the installation of indexed abutments and clearly fixes their position in relation to the frame (Fig. 29). At the time of fitting, after appropriate cleaning, the permanent abutments are finally fixed in the oral cavity. According to the manufacturer's recommendations, the torque when tightening the fixing screws should be 15 N•cm (Fig. 30).
Rice. 29. The polymer template facilitates fixation and control of the relative position of the abutments.
Rice. 30. By the time the frame is tried on, the abutments are finally installed in the oral cavity.
The minimally invasive treatment concept involves a minimum amount of manipulation of the implants and surrounding tissues. Therefore, after fitting the frame, permanent abutments remain in the oral cavity. Reducing the number of abutment changes has a positive effect on the stability and rigidity of the connection between implants and abutments.
During the fitting of the frame, in addition to the accuracy of its fixation on the abutments, the parameters of static and dynamic occlusion are monitored (Fig. 31). Then an impression with a frame is made (Fig. 32). After fixing the permanent abutments, the temporary prosthesis is re-positioned or a new one is made (Fig. 33, 34). In this case, a new temporary bridge was fabricated to further optimize the structure of the adjacent soft tissue.
Rice. 31. During fitting of the bridge frame, static and dynamic occlusion is monitored.
Rice. 32. After fitting, a cast of the jaw with a frame is made.
Rice. 33. The second temporary restoration is also made on the basis of Wax-up.
Rice. 34. Finished temporary restoration.
In the laboratory, a dental technician makes a new model. The dimensions and structure of the framework have a great influence on the durability of the restoration. All edges must be rounded. This prevents the occurrence of internal stresses in the ceramics. The thickness of the layer of facing materials should not exceed 2.5 mm. Otherwise, the risk of chipping increases sharply. Layer-by-layer cladding of the frame is carried out in accordance with the traditional rules of VMK technology (Fig. 35). This is a reliable technique that, when used correctly, can achieve very good aesthetic results.
Rice. 35. Permanent restoration with well-separated interdental spaces.
To fix the metal-ceramic bridge, temporary cement is used (Implant Temp, Swiss Quality Dental Ceramics & Implant Studio). The results of the final clinical and radiological examination indicate the complete success of complex treatment (Fig. 36, 37).
Rice. 36. Final control x-ray.
Rice. 37. Finished in situ restoration. Thanks to the formed papillae, the central incisors have a natural appearance.
Summary.
The goal of any prosthetics is to restore the functions of the dental system. To solve this problem, it is necessary to preserve and, if necessary, regenerate lost hard and soft tissues. The aesthetic characteristics of restorations are also of great importance. A comprehensive treatment concept takes into account all components of a complete dental rehabilitation, namely anatomical features, form and function.
The concept of maximum tissue protection (TissueCare) is essential for achieving predictable and long-lasting results. It involves the use of implants with a conical connection to abutments, which limits their micromobility and prevents the penetration of bacteria. The subcrestal position of the implants with an optimal surface structure and the Platform-Switching function ensures a tight fit of the bone tissue in the area where the implants connect to the abutments. This helps preserve the vestibular cortical plate and the soft tissues resting on it. All these requirements are fully satisfied by Ankylos C/X implants. Another factor that ensures that the optimal tissue structure around implants is maintained is the reduction in the number of abutment changes.
Author: Dr. Fred Bergmann, Germany
Stages of restoration with ceramic veneers
- Preparatory. The dentist performs the procedure of taking an impression of the existing dentition.
- Based on the bite, a technician in the laboratory creates a plastic model of future teeth, which is tried on the patient.
- If the patient is satisfied with the appearance of the teeth and the way they fit in the mouth, the technician makes ceramic veneers.
- Then, after grinding the patient’s teeth, the veneers are permanently bonded to the surface of the teeth.
After installation of veneers, there is no expected recovery period. The first few days the patient may feel slight discomfort due to the pads, but this quickly passes. A prerequisite for patients with veneers is regular oral hygiene and preventive examinations by the dentist.
Is it harmful to have professional whitening?
Dental clinics of the 21st century offer not just a teeth whitening procedure, but gentle procedures using systems that allow you to achieve optimal results without exposing your teeth to chemicals and acids.
In other words, due to high-quality materials, such as gels, there is a direct impact not on the tooth enamel, but not on its pigment, which is removed over time. If the gel contains hydrogen peroxide, then before bleaching, fluoridation must be done to strengthen the enamel coating. In this case, restoring the optimal appearance of your smile will be completely safe.
What are lumineers and how are they different from veneers?
Many people have heard about Lumineers, but few know what it is. Essentially, these are the same veneers, only manufactured at a factory in the USA. Lumineers is a brand of an American manufacturer that has become a household name, like Pampers or Xerox. And it is often used by dishonest dentists to promote conventional veneers. No one can make lumineers for you; they can only be ordered in the USA. We do not work with this product because, in our opinion, it is not ideal aesthetically. In appearance, such ceramics resemble sanitary ware. Making porcelain veneers in a laboratory will be much cheaper and the results will be more attractive.
Why you should sign up for Faceline
- We cooperate with the best dental laboratories in Moscow.
- We work with the most advanced ceramic veneers available today, E-Max.
- Patients are treated by experienced and qualified orthopedists Evgenia Petrovna Malykhina, Elena Nikolaevna Gordeeva, Anna Yuryevna Ermolaeva, Artem Surenovich Kochkanyan.
- We offer reasonable prices for direct and indirect dental restoration with turnkey services.
If you want to get an impeccable result from an aesthetic point of view, we invite you to Faceline Dentistry. You can find out the exact cost of treatment after making an appointment and examining a doctor.
Dental restoration with inlays
Inlays are microprostheses that restore the destroyed part of the chewing tooth. The inlay is made from an impression and then installed in the desired location. This is a more modern and durable method than restoration with composite material. The inlay is made of ceramic or zirconium dioxide and allows you to completely restore the functionality of the chewing tooth.
Indications for installation of a restoration tab:
- the surface of the molar is affected by caries;
- the molar is destroyed by more than 1/3;
- pathology, as a result of which the patient experiences increased abrasion of the enamel.
General presentation and purpose
Herculite is a unique composite material with light reflection. It has been produced for more than 20 years by the Italian company Kerr.
This enterprise began its work at the end of the 19th century. Thanks to its own developments and the addition of several leading companies from other countries, Kerr has become one of the world's largest manufacturers of consumables for dental practitioners. All products are of high quality.
Herculite technology is patented and is the world standard for restoration materials. The composite is a universal composition that recreates the natural properties of the tooth.
The substance can be used for the restoration of any dental cavities and defects:
- Filling cavities;
- Treatment of enamel erosions;
- Elimination of wedge-shaped defect;
- Correction of the shape and color of teeth;
- Restoration of ceramic dentures.
"Denta-Professional" - we work to make you smile
Our clinic has existed since 1999. We solve any dental problems, regardless of their complexity. "Denta-Professional" is:
- Professionals with experience. We employ only highly qualified doctors who regularly undergo advanced training courses and master new working methods.
- Safety. We carefully comply with all existing sanitary standards to provide our patients with the best conditions. All reusable instruments are disinfected, and disposable ones are disposed of after use.
- Individual approach. We select the course of treatment, the necessary materials, and anesthesia based on the physiological characteristics of the patient. It is important to us that any procedure is not only successful, but also effective.
- Guarantees. We provide a guarantee of up to 5 years for the work we perform. If during the warranty period anything happens to the installed fillings or other materials, we will repeat the procedure free of charge.
Sign up for a consultation now.
Visit to the dentist without pain
Forget the stress of a botched anesthesia, FDC uses painless pain management techniques.
QuickSleeper is an electronic system that provides simple, fast and comfortable pain relief.
VibraJect is a special attachment.
It is an effective way to reduce pain and anxiety during local anesthesia. All this helps reduce patient stress from painful injections and unpleasant visits. Read more about painless anesthesia with QuickSleeper
Teeth whitening at CELT
Thanks to the latest version of the popular in-office whitening system, “Zoom 4” from Philips, dark tooth enamel and the appearance of stains on it from the consumption of coloring products are no longer a problem. The essence of the technique with its use is to apply a gel with hydrogen peroxide and potassium phosphate to the tooth surface. It begins to act under the influence of ultraviolet light: oxygen molecules that are released in the process penetrate into dental tissue and destroy coloring pigments. Due to this, the whitening effect is achieved.
The “Zoom 4” whitening procedure at CELT has a number of advantages:
- It is absolutely safe for the patient’s body;
- Will not cause discomfort;
- Lasts only 45 minutes (several cycles of 10 minutes);
- The risk of overheating of dental tissues during the procedure is eliminated;
- The composition includes “Relief” gel, which reduces tooth sensitivity.
The esthetician first applies a protective composition to the gums, then a whitening gel to the teeth, which is activated by directing UV rays at it. Upon completion of the procedure, he removes the gel and protective composition and evaluates the result. In order to keep your teeth white for a long time, you will have to limit your consumption of products with coloring pigments.
Restoration with veneers and lumineers
Veneers and lumineers are thin but very durable shells made of ceramic, porcelain or zirconium. Plates are placed on the outside of your teeth in order to change their shape, position, and hide an unsightly shade.
In the photo you can see how the frontal appearance of the teeth has changed after using onlays.
Veneers and lumineers differ in thickness, installation method, service life and price. Lumineers are thinner and do not require preliminary grinding of teeth before installation (unlike thicker veneers). If they are removed, the teeth will remain undamaged. Lumineers are created only in America, they are produced under the Cerinate or DUO brand. The price for them is quite high. They will last 20-25 years, while veneers will last about 5-7 years on the teeth.
The duration of treatment depends on the timing of production of the onlays. On average, their production takes from one to four weeks.
Important! The structures cannot withstand strong pressure and can come off under excessive load. Therefore, it is advisable to install them only on the front teeth, which include the canine and incisor, because their main purpose is more the aesthetics of a smile, and not chewing food.
Stages of treatment
Aesthetic restoration of the anterior teeth takes place in 2 stages, since it is an indirect method of treatment:
| First stage | Second phase |
|
|
Main advantages of the method
- elimination of all visible dental defects;
- acquiring a healthy and beautiful smile;
- painless installation (no anesthetics required);
- hypoallergenic;
- durability;
- ease of care;
- maintaining natural whiteness throughout its entire service life.
Restoring aesthetics using lumineers and veneers has disadvantages; they are associated with the fragility of the structures and the need to restore ground teeth if the onlays had to be removed (associated only with veneers). If you have onlays in your mouth, it is recommended to carefully monitor your diet and control bad habits so as not to damage the microprostheses. You should not eat solid foods whole, or chew nuts with your teeth, open lids, or bite off threads.
Note! Even if the lining is slightly damaged, it will not be repairable and will need to be replaced. Therefore, veneers and lumineers are not installed in cases where a person leads a traumatic lifestyle or engages in professional sports, such as boxing.
How much does the restoration cost?
The final cost of restoration is influenced by many factors. The price depends on:
- materials used to carry out the process;
- preliminary preparation of teeth: often it is necessary to pre-treat them, clean the canals, get rid of old fillings, etc.;
- the method chosen to perform the manipulations;
- type of anesthesia;
- size of the carious area;
- the level of the specialist and the clinic in which he provides his services.
The most affordable restoration is made from photopolymer materials. Others have a higher cost, therefore the procedure itself is more expensive. To find out how much money you need to spend on restoration, you need to consult a dentist. He will offer and advise various materials and techniques. Based on this, the specialist will adjust the total cost that is optimal for a particular patient. You need to understand that high-quality material cannot cost little.
Materials
Photopolymer materials that are used in direct restoration have become widespread. In this case, a high result is guaranteed. The fact is that, for example, fillings that are made of photopolymer materials almost never fall out, and they can also be easily selected by color based on the shade of the enamel.
In this way, teeth are restored in layers, due to which the anatomical structure of the tooth is completely restored. Each layer is dried under the lamp. Thanks to this method, prosthetics can be avoided. Moreover, this method has many advantages. For example, the durability of artistic restoration is the same as that of many types of prosthetics. But the person retains his teeth, which become very beautiful. Composite materials are also very popular. They mainly contain special fillers. In order to seal chewing teeth, large particles are often used. Small ones are for restoration. They have less strength, but boast excellent characteristics.
Heliocomposite is a material that is widely used in dentistry. You can easily and accurately make a model of any tooth from it. To make it hard, use a gel lamp. The variety of different shades allows you to choose any color. There are a huge number of variations of this material. There are complex composites that are used in the manufacture of inlays and veneers.