What is a tooth fracture? This is damage to the integrity of the anatomical structure of the tooth. The supragingival or subgingival part of the tooth may break (break or chip), damaging dentin, cement or enamel. Most often, a tooth fracture occurs due to blows or falls, with damage to the face. Less often, this occurs due to the inclusion of small solid objects in food (small pebbles in buckwheat or rice).
Classification
Depending on the part of the tooth in which the fracture occurred, there are:
- tooth root fracture
- fracture of the coronal part of the tooth exposing the pulp
- fracture of the coronal part of the tooth without exposing the pulp
Symptoms
When a tooth root is fractured, a sharp pain occurs when touching the tooth, the crown part of the tooth becomes mobile, the final diagnosis is made after a targeted x-ray. If there is a fracture of the coronal (visible) part of the tooth with exposure of the pulp, then the tooth becomes sensitive to thermal and chemical stimuli, but the tooth is motionless. When a tooth is fractured without exposing the pulp, an aesthetic defect in the tooth crown occurs; the tooth is stable and does not respond to cold or heat.
Treatment method
If the root is fractured in the area of the tooth neck, at the gum level, the root canals of the tooth are filled, then a stump inlay and then a metal-ceramic crown are installed in the root of the tooth. If the root fracture passes below the neck of the tooth, then the entire tooth is removed.
Deputy Chief physician Sergey Evgenievich Brodsky
Sign up for a free consultation
+7
When the coronal part of a tooth is broken off with exposure of the pulp, the tooth is depulped and the tooth is subsequently restored with composite fillings or ceramic inlays. When, as a result of a fracture of the coronal part of the tooth, the dental pulp is not exposed, the tooth is restored with ceramic inlays or composite restorations.
Just CALL US!
+7
We will answer any of your questions and will definitely help you!
Causes
There are several reasons for the occurrence of tooth crown fractures. They are caused by:
- habit of biting pens, opening bottles with teeth, etc.,
- regular consumption of very solid foods - nuts, crackers,
- temperature fluctuations - alternation of hot and very cold food,
- the presence of large fillings that do not have support,
- piercing of soft tissues of the oral cavity - tongue, cheeks, lips.
The combination of several risk factors increases the likelihood of tooth cracking. To notice damage in time, you need to undergo regular dental checkups.
Complications after surgery
The most common complications encountered by patients who have undergone tooth root removal surgery are severe bleeding and alveolitis. Factors that can trigger bleeding include high blood pressure or decreased blood clotting. In turn, the main cause of alveolitis is non-compliance with the postoperative regimen, leading to the washing out of the protective blood clot from the socket. The development of the disease is accompanied by the occurrence of an inflammatory process, suppuration of the wound formed during the removal of the tooth root, the appearance of pain and bad breath.
Manifestations
In most cases, cracks on the tooth form gradually and at the first stage are very small in size. Violation of the integrity of the crown may be indicated by:
- hypersensitivity when eating hot and cold foods - coffee, tea, ice cream,
- discomfort when leaving a warm room into the cold,
- pain during chewing.
If these signs appear, you should not postpone a visit to a specialist. The sooner a fracture is detected, the easier it is to solve the problem and maintain dental health.
Procedure for removing tooth roots
The tooth root extraction operation is performed under local anesthesia. Before starting the procedure, the surgeon carefully studies the results of the X-ray examination. The information obtained from analyzing the image helps the doctor plan the course of the operation and select the necessary tools.
During surgery the following can be used:
- forceps;
- elevator;
- dental bur.
Extracting a tooth root using forceps
In the first case, the operation begins with careful separation of the gums and other tightly adjacent tissues from the root remaining in the jaw tissue. Then the doctor places forceps on the root part of the tooth and pushes their cheeks under the gum tissue, trying to grasp the unit to be extracted as tightly as possible. A well-fixed root is dislocated using rocking or rotating movements and carefully removed from the alveolar socket.
Carrying out operations using elevators
Elevators are used in cases where there are no conditions for removing it with forceps (for example, when it is located deep in the alveolar socket). The doctor carefully peels away the tissue adjacent to the remaining tooth, inserts an elevator into the space between the alveolar wall and the unit to be removed and, using the tool as a lever, gently dislocates the root. When the root part becomes mobile, the surgeon removes it from the socket using forceps.
Cutting out the root with a bur
If there are no conditions for root removal using standard instruments, alveolotomy is performed - a surgical intervention that involves destruction of the outer wall of the alveolar socket.
This operation is carried out in several stages and includes:
- incision of the gums and subsequent delamination of the mucoperiosteal tissues in the area of surgical intervention;
- cutting the outer wall of the alveolar socket with a bur and exposing the root;
- insertion into the resulting passage of the elevator and careful dislocation of the remaining tooth;
- root extraction from the alveoli;
- grinding the pointed edges of the alveolar socket;
- careful suturing of the wound.
The duration of the tooth root removal operation can vary from several minutes to 2-3 hours.
Diagnostic and treatment methods
To detect tooth crown fractures and determine their sizes, several methods are used:
- visual inspection,
- coating of enamel with dyes,
- drying of the tooth
- radiography,
- if necessary - CT.
Based on the examination results, the doctor chooses a treatment method. The choice depends on the location and depth of the crack.
- The enamel structures are covered with a composite material.
- If the crack affects the dentin, the tooth is restored. If the pulp is damaged, endodontic treatment is required.
- A large defect needs excision. The damaged tissue is removed, the tooth is prepared and covered with a crown. It is possible to install a pin.
If the fracture affects the bottom of the pulp chamber, the tooth cannot be saved. The damage in this case is accompanied by pulpitis and periodontitis. The problem can be solved by planned tooth extraction followed by prosthetics or implantation.
VERTICAL CRACK OF THE TOOTH ROOT. ETIOLOGY, CLINICAL SYMPTOMS, DIAGNOSIS
Published in 2016, Issue December 2016, MEDICAL SCIENCES | No comments yet
Makeeva I.M.¹, Byakova S.F.², Adzhieva E.K.³
¹Doctor of Medical Sciences, Professor, Head. department therapeutic dentistry PMSMU named after. M.I. Sechenov in Moscow,
²Candidate of Medical Sciences, Associate Professor of the department. therapeutic dentistry PMSMU named after. THEM. Sechenov in Moscow,
³Applicant department therapeutic dentistry Perm State Medical University named after I.M. Sechenov in Moscow
VERTICAL CRACK OF THE TOOTH ROOT. ETIOLOGY, CLINICAL SYMPTOMS, DIAGNOSIS
annotation
One of the most unfavorable complications in root canal therapy is vertical root fissure (VRF) in endodontically treated teeth. The prognosis of such teeth is most often hopeless and differential diagnosis from other endodontic complications can be difficult. However, making an accurate diagnosis is very important in order to distinguish vertical root fissure from other post-endodontic conditions. Our study describes more typical clinical and radiological features.
Key words: vertical crack of the tooth root, vertical tooth fracture, endodontics, post-endodontic complication.
Makeeva I. _ M.¹ , Byakova S. _ F.² , Adzhieva E. _ K.³ _
¹MD, professor, Head of Department of Theurapy Dentistry, IM Sechenov First Moscow State Medical University,
² MD, Assistant professor of Department of Theurapy Dentistry, IM Sechenov First Moscow State Medical University,
³Postgraduate student of Department of Theurapy Dentistry, IM Sechenov First Moscow State Medical University
VERTICAL ROOT FRACTURE. ETIOLOGY. CLINICAL SYMPTOMS. DIAGNOSTICS
Abstract
A most frustrating complication to root canal therapy is vertical root fracture (VRF) in an endodontically treated tooth. Prognosis most often is hopeless and differential diagnosis from other pathoses may be difficult at times. However, proper diagnosis is critical to distinguish a fracture complication from clinical manifestations of periodontal and endodontic diseases. Our research emphasizes the importance of the correct diagnosis of VRF, describes the more typical clinical and radiographic features of this disorder.
Keywords: vertical root fracture , endodontic treatment, postendodontic disease.
For the first time, the term “vertical root fracture” appeared in foreign literature and is translated into Russian as “vertical root fracture”, “vertical root fracture”, “longitudinal root fracture”, etc. In our work we considered vertical root fissure (VRC) as a complication of endodontic treatment, characterized by the gradual development and emergence of a focus of destruction of the adjacent bone tissue. [7, 8]
A vertical root crack can occur both during endodontic treatment, under the pressure of a “propping” force on the canal walls during gutta-percha condensation [5, 6, 7, 8], and subsequently, under the influence of occlusal load, during fixation of anchor pins and stump inlays [3]. Also, a vertical crack in the roots of the teeth can be caused by restoration of the coronal part of the tooth: excessive removal of hard tissues during the formation of the cavity, improper formation of the occlusal surface of the tooth, an increase in the chewing surface of the tooth, the presence of amalgam fillings, etc. [4].
The anatomical features of certain groups of teeth make them more susceptible to the occurrence of VTK. Most often they occur in the roots of the premolars of the upper and lower jaws, the mesial roots of the molars of the lower jaw, and the mesiobuccal roots of the upper molars [2, 7, 8].
Making a diagnosis of “vertical tooth root crack” is difficult. The complexity of diagnosis is explained by the fact that with vertical root fractures, the complaints, clinical and radiological picture are similar to those with periodontal diseases and apical periodontitis [7, 8, 9]. In most cases, symptoms of VTC appear 1-2 years after its formation and are not specific, because observed in many other post-endodontic conditions [7,10].
According to the analysis of more typical symptoms characteristic of VTK, there are complaints of discomfort and pain, aggravated by biting, swelling, the presence of a fistula, and slight tooth mobility [1, 7]. The triad of symptoms that have been proposed as “pathognomonic” for a vertical root fissure (endodontically treated tooth, high fistulous tract, narrow deep periodontal pocket) is not present in all cases of vertical root fissure [8]. As a rule, it is possible to establish a diagnosis only if there is a significant focus of bone destruction with a characteristic localization, or with visual confirmation of the presence of a crack after it has spread to the coronal part of the tooth.
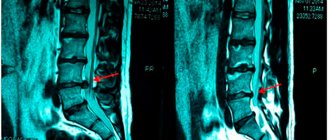
Intraoral contact radiography makes it possible to make an accurate diagnosis of VTK of teeth if the fracture line is visible, which, as a rule, is determined when the direction of the X-ray beam coincides with the plane of the crack. At the same time, this diagnosis is complicated by the display of multi-rooted teeth, due to the overlap of several projections of the tooth roots [11].
The prognosis of teeth with VTK is unfavorable, and, as a rule, extraction is the only possible treatment option. Early diagnosis is extremely important, since in the presence of a root crack, an infectious process develops in the adjacent periodontal tissues, which leads to rapid destruction of the alveolar bone
The purpose of our study was to improve the diagnostic performance of vertical root cracks based on clinical characteristics and radiographic examination.
The study was conducted by questioning dental surgeons who removed teeth diagnosed with a vertical root crack. The following tasks were set:
- Identify risk factors for this pathology, the most common causes characteristic of the clinical signs of VTC pathology;
- Analyze the information content of targeted radiography
To solve these problems, we have compiled a questionnaire for dental surgeons. 84 questionnaires were sent to dental surgeons at the departments of the I.M. Sechenov First Moscow State Medical University.
Doctors were aware of some typical symptoms of VTC teeth, such as: deep, narrow periodontal pocket; characteristic fistulous tract near the gingival margin; periapical changes in a targeted X-ray image in the form of a “halo”. This information allowed them to be wary of identifying teeth with VTC and helped them fill out the questionnaire.
The questionnaire consisted of 9 questions concerning both the tooth being removed directly and other factors that are often the background to the occurrence of VTC.
Considered:
- Patient's gender.
- Age.
- Overload factors with several sub-items taking into account the presence of traumatic occlusion and bruxism.
A dental formula that reflected the condition of each tooth (presence of fillings, crowns, etc.) Separately in the dental formula, the tooth under study, aimed for removal, was noted.
- Number of the tooth to be removed, diagnosis (if referred).
- Patient complaints.
- Clinical characteristics: presence of a periodontal pocket, abscess, fistula, description of them if any.
- X-ray data of targeted radiography.
- Characteristics of the tooth: assessment of endodontic treatment of the canal – expanded within normal limits/excessively expanded.
Availability of orthopedic structures: crown; stump pin insert; anchor pin; description of them in relation to the tooth root canal.
- Time of tooth functioning after previous endodontic/orthopedic treatment.
Considering that the maximum information about the topography and condition of the roots of teeth can be obtained in the case of polypositional radiography, targeted radiography was carried out in three projections:
- straight – with orthoradial beam direction;
- posterior oblique – distal eccentric direction of the beam;
- anterior oblique – mesially eccentric direction of the beam.
Dental surgeons participating in this study filled out the provided questionnaires after tooth extraction, visually confirming the diagnosis of “vertical root fissure”, because Teeth with VTC are often removed due to the presence of other pathologies accompanying this diagnosis (such as bone loss, deep periodontal pockets, etc.). The cause of these pathologies, in this case the diagnosis of “vertical root crack,” was already made after tooth extraction.
An analysis of questionnaires from 84 clinical cases conducted by dental surgeons showed that in 65.4% of cases, a referral for removal was indicated by a diagnosis of apical periodontitis. In the remaining 34.5% (29 teeth) a vertical crack of the tooth root was diagnosed. Of these, 19% (16 cases) of VTK were detected on targeted radiography (in direct projection), in 9% (8 cases) VTK was detected using the diagnostic operation “detachment of the flap”.
Patients who applied mainly complained of discomfort (94.04%). Pain when biting was noted in 75%. A periodontal pocket with periodic suppuration was observed in 40 cases (47.6%) and had a characteristic shape - narrow, which required probing along the entire perimeter of the tooth neck to detect. Pain, swelling and redness of the gums were noted in 43 cases (51.1%). The presence of fistula in 14 cases (16.6%), with a characteristic feature of location at the gingival margin (Fig. 1). In 82.1% of cases, VTC had a vestibulo-oral direction. Periodontal pockets and areas of bone destruction formed as a result of the presence of vertical root cracks were either the only ones or did not correspond in severity to other areas of the inflammatory-destructive process. The results of clinical characteristics are presented in Table 1.
Table 1 – the most typical symptoms and clinical characteristics of VTC.
Figure 1: a – location of the fistula tract with VTK of 34 teeth; b – targeted radiograph of gutta-percha along the fistula at the 34th tooth; c – removed 34th tooth with VTK.
In all 84 cases (100%), teeth with a vertical root crack had previously been treated endodontically. In 40 cases (47.6%) excessive expansion of the root canals was noted. Moreover, in 94% of cases, the service life after endodontic treatment was more than one year, 5.9% - less than a year. A large number of dental implants were observed in teeth with pin and stump inlays - 55.9%, while in 35.7% of cases excessive preparation of hard dental tissues was noted during the manufacture of these orthopedic structures.
In 65 cases (77.3%) there was occlusal overload. At the same time, in 29.7% - the presence of bruxism, 11.9% - the use of a tooth as a support for a bridge, 11.9% - a support for a removable denture, as well as in secondary adentia with the loss of a significant number of teeth with the absence of rational prosthetics - 23 ,8%. The results for occlusal overload factors are presented in Table 2.
Table 2 – Results on the influence of overload factors
In 28.5% (24 cases), a vertical crack in the tooth root was diagnosed on a targeted radiograph, based on the presence of a fracture line along the longitudinal axis of the tooth. In 35.7% (30 cases) of tooth VTC displays on a targeted radiograph, periapical changes had characteristic signs - a defect in the form of a “halo” in the area of one of the lateral sides of the tooth, tapering towards the apex.
Of the total number of extracted teeth with a vertical root crack, in 34.5% (29 cases) VTC was diagnosed primarily, being the reason for the removal. In the remaining 65.4% (55 cases), only indirect signs indicated a crack, and the reason for referral for removal was a diagnosis of apical periodontitis.
In our study, a vertical crack in the root of a tooth was found in previously endodontically treated teeth in 100% of cases. It should be noted that in almost half of cases of VTK there is excessive expansion of the root canals. More than half of the cases occur with the use of pin structures. Therefore, when making a diagnosis, these factors should be taken into account, together with complaints and clinical manifestations. Of the clinical characteristics for this pathology, the most characteristic is a high fistulous tract and a narrow periodontal pocket. Using the method of targeted radiography, it is possible to diagnose no more than 1/3 of all vertical cracks in the roots of teeth, taking into account the polypositional method of this diagnosis.
A vertical root crack still causes great difficulties in diagnosis. But making a diagnosis and removing a tooth with VTK is the method of choice in the outcome of this pathology.
List of literature / References
- Chan S. P. Vertical root fracture in non-endodontically treated teeth-a clinical report of 64 cases in Chinese patients / P. Chan, SCTseng, CPLin // JEndod. – 1998. – Vol. 24 – No. 10. – P. 678-81. doi: 10.1016/j.joen.2009.09.013.
- Cohen S. Vertical root fractures – clinical and radiographic diagnosis / S. Cohen, L. Blanco, L. Berman. // J Am Dent Assoc 2003. – No. 134 – P.434–441. – doi:10.14219/jada.archive.1983.0276.
- 3. Lertchirakarn V. Patterns of vertical root fracture factors: affecting stress distribution in the root canal / V. Lertchirakarn, JE Palamara, HH Messer // J Endod – 2003. – Vol.29 – No. 8 – P.523-528. – doi:10.1097/00004770-200308000-00008.
- Lommel TJ Diagnosis of possible causes of vertical root fractures / TJ Lommel, F. Meister, H. Gerstin // Oral Pathol Oral Med Oral Surg. – 1980. –49 – No. 3 – P.243. –doi: 10.1016/0030-4220(80)90056-0.
- Ozer SY Detection of vertical root fractures of different thicknesses in endodontically enlarged teeth by cone beam computed tomography versus digital radiography / Journal of Endodontics. – 2010. –36 – P.1245–9. – doi: 10.1016/j.joen.2010.03.021.
- Silveira P.F. Detection of vertical root fractures by conventional radiographic examination and cone beam computed tomography – an in vitro analysis/ PFSilveira, MBVizzotto, GSLiedke and others // Journal of Endodontics – – Vol. 29 – No. 41 –P.6. – doi: 10.1111/j.1600-9657.2012.01126.
- Tamse A. Vertical root fractures in endodontically treated teeth: diagnostic signs and clinical management // Endodontic topics. – 2006. – Vol.13 – P. 84-94. – doi: 10.1111/j.1601-1546.2006.00200.
- Tamse A. Vertical root fractures in dentistry/ A. Tamse, I. Tsesis, E Rosen // Switserland, Springer international publishing – 2015 – P. 133. – doi: 10.1111/iej.12109.
- Tamse A. Radiographic features of vertically fractured endodontically treated maxillary premolars / A. Tamse, Z. Fuss, JP Lustig and others // Oral Surg Oral Med Oral Pathol Oral Radiol Endod – 1999. – Vol.88 – P.348–352. – doi: 10.1016/s1079-2104(99)70041-7
- Tamse A. Radiographic features of vertically fractured endodontically treated mesial roots of mandibular molars/ A.Tamse, Kaffe, J. Lustig and others // Oral Surg Oral Med Oral Pathol Oral Radiol Endod – 2006. – Vol.101 – P.797– 802. – doi: 10.1016/j.tripleo.2005.09.014
- Youssefzadeh S. Dental vertical root fractures: value of CT in detection.Radiology/ A.Gahleitner, R.Dorffner, T.Bernhart // Journal of Endodontics – 1999. –210 – P.545–549p. – doi: 10.1148/radiology.210.2.r99ja20545
Filling materials
A hermetic seal is created by a combination of modern materials:
• Gutta-percha in the form of a dense pin. The homogeneous structure and thermoplastic characteristics of the natural material make it possible to obtain a homogeneous filling that adapts to any root canal.
• Sealer, cement layer. The material increases the strength of the filling by sealing the space between the walls of the root canal and the gutta-percha.
Seals made from these materials meet the following requirements:
– seal the root and its branches;
– create a favorable environment for the regeneration of root tissues;
– correspond to the channel configuration;
– do not irritate surrounding tissues;
– protect against pathogens, prevent their penetration into the root canal.
Types of dental crowns for chewing teeth
When choosing a material for creating a microprosthesis, you should take into account the functional purpose of the teeth.
The molars of the posterior zone of the dentofacial apparatus are subjected to strong mechanical and chemical stress when chewing food. Eating food that differs in taste, composition and hardness can quickly damage the nozzle, which is made of aesthetic material, but vulnerable to the abrasive properties of some products. In addition, the material should not cause allergies to the soft tissues of the oral cavity. Therefore, it is better to entrust the choice of material to a specialist. I am an orthopedic dentist, Sergey Samsakov, taking into account the results of the research, I recommend the optimal material option for creating a crown in each specific case:
- Metal-ceramic crowns
- a successful combination of strength, cost and beauty have made this type of onlay the most popular for installation on a tooth. Metal-ceramic crowns are installed with mandatory circular grinding of the tooth being restored.
- Metal crowns
are reliable products with a budget price. These are long-term onlays with good biological compatibility and do not require preparation of healthy tooth tissue. They can be made in combination with precious alloys. The only negative is the possibility of developing an allergic reaction. - Ceramic prostheses made of zirconium dioxide
are an ideal option for placing crowns in patients with contraindications to the use of metal structures. The high cost of the ZrO2 crown is fully compensated by the durability and aesthetics of the dentition. - Metal-plastic
dental prostheses are very fragile and are used by the doctor as temporary crowns on a tooth with the subsequent installation of a permanent crown made of durable material.
The structural reliability of the prosthesis allows you to protect the living tooth from further abrasive processes and maintain the ability to fulfill its purpose - thoroughly chewing food.