Implantation is a technology that allows you to successfully restore teeth in a variety of cases - both when it is necessary to eliminate a single defect in the dentition and when a person is missing all the teeth in the rows. When carrying out implantation, special designs are used - implants implanted into the jaw bone. When the implants take root and completely fuse with the bone, a prosthesis is placed on them.
Implantologists call the moment of installation of a prosthesis on an implant a load, and the loading of implants with a prosthesis can be either immediate or delayed. What is implantation with immediate loading, what are its features, advantages - we will tell you about this in this article. We will find out and consider the indications and contraindications for implantation with immediate loading and provide approximate prices for the service in Moscow.
Calculate the cost of treatment by taking a short test in 20 seconds!
Do not delay your treatment, because in this matter time plays against us.
What is immediate loading implantation?
Implantation with immediate loading is an implantation whose protocol will involve the installation of a prosthesis on the implants almost immediately after their implantation. Usually - two to three hours after installing titanium rods in the jaw bone, sometimes - 2-3 days after surgery. Since the installation of implants and their immediate loading with a prosthesis are carried out in one stage, such implantation is often called one-stage implantation.
WORTH KNOWING AND REMEMBERING: Single-stage implantation is often confused with one-stage technology for installing implants. The difference is that, although simultaneous implantation also uses immediate loading of the implants with a prosthesis, it involves installing implants immediately after tooth extraction, directly into the hole remaining after extraction (removal) of the tooth from the jaw.
During implantation with immediate loading, temporary plastic prostheses are placed on the implants. A person will use them until the implants fully and efficiently fuse with the natural tissue of the jaw. After the osseointegration process of the implants is completed, the temporary prosthesis is replaced with a permanent crown.
Immediate loading with a prosthesis is also used when it is necessary to eliminate a single defect in the dentition and, if necessary, urgently restore all teeth at once. The all-on-4, all-on-6 implantation protocols use immediate loading with a prosthesis, which allows you to extremely quickly solve the problem of complete edentia.
BY CHEWING YOUR FOOD YOU HELP THE IMPLANTS TAKE PLACE
Instant chewing load is one of the key points of the technology, since implants act as conductors of chewing load, capillaries in bone tissue are activated, cells begin to receive proper nutrition and self-heal. Thus, in addition to restoring aesthetics and returning to normal food intake, patients also help the process of osseointegration (engraftment of implants in the body). In patients with severe facial asymmetry due to missing teeth, the bite is gradually restored, the facial muscles begin to work as before, and premature signs of aging disappear. Diction is restored, digestion and the general condition of the body as a whole are improved. The fact is that due to the absence of teeth, patients begin to avoid hard foods; as a result, less nutrients enter the body and metabolism is disrupted.
Advantages of implantation with immediate loading
The main advantage of implantation with immediate loading is that it allows you to quickly eliminate a defect in the dentition and relieve a person from psychological discomfort and the need to somehow limit oneself in nutrition. This technique is recommended when it is necessary to quickly restore teeth, either completely, or one or more units included in the smile area.
Also among the advantages of implantation with immediate loading:
- Installation of implants and their immediate loading with a prosthesis - these activities are carried out in one operation;
- Reduced invasiveness of implantation for the patient. When implanting with immediate loading, special implants are used that are integral with the abutment. The entire structure is placed into the jaw bone at one time and onto it and given immediate load with a temporary prosthesis. In two-stage implantation, dismountable implants are used: in the first stage, the implant itself is placed, and the incision on the gum is sutured. After the implant has taken root, the gum is cut again, the former and abutment are placed, and only then the prosthesis is installed;
- Immediate load on the prosthesis has a positive effect on the rate of implant healing. Thanks to immediate loading, implants quickly fuse with the jaw bone;
- Since during implantation with immediate loading, surgical manipulations are minimized, the rehabilitation process is faster.
But implantation with immediate loading also has disadvantages. The most important disadvantage of dental implantation with immediate loading is the increased risk of implant rejection, which occurs because the implanted artificial root will almost immediately be subject to strong pressure from the installed prosthesis. If you incorrectly calculate the degree of this pressure when planning implantation with immediate loading and also choose the wrong implants, the implanted titanium rod may not take root, and the process of its rejection will begin. The correct choice of dentistry for treatment will help reduce the risk of implant rejection after implantation with immediate loading.
The well-equipped clinic has all the necessary equipment that allows you to plan implantation with immediate loading so as to completely eliminate possible risks to the health of patients. The utmost attention is paid to planning and detailed development of implantation in our VENSTOM dentistry in Moscow!
The disadvantages of implantation with immediate loading include a large number of contraindications, which definitely need to be excluded at the stage of preparation for treatment. When is it impossible to perform implantation with immediate loading? We will tell you about this in the next section of our article.
Advantages of the basal implantation method
The unique feature of the method is determined by the method of implanting implants into the deep basal layers. These tissues are practically not subject to atrophic processes, unlike the alveolar spongy layer. As a result, it is possible to install implants using the basal method even in complex clinical cases, when alveolar tissues are atrophied, in patients with periodontal disease and other serious diseases.
Installation is carried out using the compression method through a puncture. This is a much less traumatic method compared to the need to saw through the bone for a plate implant or remove a flap of gum for a two-phase implantation.
Basal implantation is performed using monoblock systems, that is, the rod and abutment form a single whole. This made instant loading possible: immediately after implantation, a light bridge-like prosthesis is fixed on the top of the implant and included in the chewing process.
Being correct load conductors, such implants transfer normal pressure when chewing food to the bone layers of the jaw. This stimulates metabolic processes in them and activates osseointegration.
Due to the fact that the implant and abutment are a one-piece structure, FIXED dentures can be installed immediately. A person can forget about missing teeth or removable dentures, returning to a normal lifestyle within 3-4 days. Implants, being conductors, evenly and correctly distribute pressure on the bone and among themselves, while stabilizing each other. The implant healing process is based on stimulating the natural processes of bone tissue restoration during the process of chewing food.
Indications and contraindications for immediate loading dental implantation
Any medical procedure or operation has both indications and contraindications for use. Implantation with immediate loading is no exception in this regard, and if we talk about indications, then this implantation protocol is used:
- 1. If it is necessary to quickly restore all teeth in the jaw (with complete edentia).
- 2. When you urgently need to restore 3-4 missing teeth in a row.
But if you only have one tooth missing, then the doctor will decide on the possibility of implantation with immediate loading on an individual basis.
To achieve excellent primary stability of the implants, which will allow immediate loading of the prosthesis, the structures are implanted into the bone at an angle. If a person has healthy teeth in his mouth next to the defect, then it is not always possible to install an implant in the desired position: the risks of damage to the root part of healthy teeth are too high. Therefore, implantation with immediate loading in the absence of only 1 tooth is rarely performed. The possibility of carrying it out and applying immediate load to the implants with a temporary crown will be determined by the doctor after a diagnosis, including a CT scan of the jaw.
There are many more contraindications to implantation with immediate loading than indications. Let's look at situations in which it is impossible to install implants with immediate loading:
- 1. Implantation with immediate loading requires good bone tissue. To put an immediate load on the implant, it is necessary to obtain its excellent primary stability in the bone, which is unattainable if the bone tissue is loose and does not have sufficient height and volume. If bone deficiency is observed in the upper jaw, then zygomatic implants can be used for immediate loading implantation, thereby eliminating the need for preliminary bone grafting. But if the lower jaw bone has atrophied, implantation with immediate loading is not carried out.
- 2. Implantation with immediate loading cannot be carried out even if the tooth was removed inaccurately and this led to damage to the jaw bone or the formation of a socket that was too wide.
- 3. For oncological diseases, pathologies that cause destruction of bone tissue, disorders of blood clotting processes.
All these contraindications must be excluded at the very first stages of treatment, and for this it is important to carry out a thorough and thorough diagnosis! In our dental clinic in Moscow VENSTOM, implantation is planned based on accurate diagnostics carried out using modern equipment!
Doctor's advice: an implant can only be installed if the bone size is sufficient.
In all cases, the parameters of bone tissue are taken into account - density, height, width. Only when there is sufficient bone size can an implant be installed with a selected size and shape that can cope with chewing loads in the future. If there is not enough bone tissue, it is impossible to install the “correct” implant.
Levin Dmitry Valerievich
Chief physician, Ph.D.
If the bone dimensions do not correspond to the norm, preliminary osteoplasty is required, followed by installation of an implant according to the classical protocol. If the deficiency is small, a one-step bone augmentation and implant installation is possible.
A high-quality one-stage technique cannot be carried out in conditions of insufficient bone tissue. And it is also impossible to carry out bone augmentation at the same time - the operation is performed through a puncture, the doctor does not have access to the bone, he places the implant blindly.
In addition, with a one-stage protocol, the implant is immediately loaded with a temporary crown, which does not completely compensate for chewing functions. The implant cannot be actively used to avoid displacement. Full load is possible only after engraftment of the titanium root after 2-6 months, as with the classical method.
Complete restoration of chewing ability is no different for the classic and one-stage protocols. One-stage allows you to quickly hide an aesthetic defect, which is only relevant for the front teeth.
Classic implantation lasts longer, especially if the bone is previously built up. But the method is reliable and designed for long-term results:
- an implant of the correct shape and size is selected;
- before engraftment, it is sutured, overgrown with bone tissue, and not loaded—the risk of displacement during chewing is eliminated;
- during installation, the doctor sees the area of the operation and can perform manipulations to adapt the bone to future loads - this is impossible with immediate loading.
How is immediate loading implantation performed?
Treatment begins with a visit to the dental clinic and consultation with an implantologist. At a consultation appointment, the implantologist conducts an examination and prescribes a series of diagnostic examinations that will determine the patient’s general health and see the condition of the jaw bone tissue.
Based on the diagnostic data, the implantation technique is selected (for example, in case of complete edentia, the “all on four” protocol is used) and the implants themselves, which will be installed in the bone. A detailed plan for the upcoming implantation is drawn up, after which preparations for the installation of implants begin.
Before installing implants into the bone, it is important to treat all teeth affected by caries, and also be sure to undergo a professional oral hygiene procedure.
WORTH LEARNING AND REMEMBERING: Why is it so important that high-quality sanitation of the oral cavity is carried out before installing implants? It's simple: plaque and tartar are the most pleasant environment for the development and reproduction of bacteria. If these bacteria get to the implant, an inflammatory process will begin, due to which the titanium rod may be rejected.
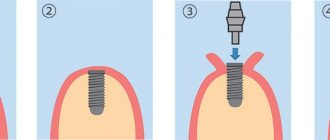
The operation itself to install implants with immediate loading goes like this:
- 1. The area where the implants are installed is numbed. Local anesthetics are usually used for this purpose.
- 2. The implantologist creates access to the jaw bone (this is done by puncture) and forms a depression in it, into which the implant with an abutment is inserted.
- 3. A temporary crown is attached to the implant abutment.
There is a break in the treatment process until the implant is completely osseointegrated. When the osseointegration process is complete, the temporary prosthesis on the implant is replaced with a permanent crown. On average, the stage of permanent prosthetics after implantation with immediate loading is carried out after 3-5 months.
Which is better: implantation with immediate loading or classic implantation with delayed loading?
It is incorrect to answer such a question in absentia, because the implantation technique and the type of load on the implants are always chosen individually for each patient. Therefore, this question can only be answered after visiting the clinic and conducting diagnostics, which will show the condition of the bone tissue and allow you to choose the optimal implantation technique for you.
For patients with a completely toothless jaw, implantation with immediate loading (in the absence of absolute contraindications) will be one of the most cost-effective options for restoring dentition. It will be carried out using “all on four” or “all on six” technologies, which imply the use of a minimum number of implants - hence significant savings, because the more implants are used in dental restoration, the more expensive the implantation is for the patient.
Is the immediate loading implantation technique right for you? Come to our dentistry in Moscow - VENSTOM - and our specialists will answer in detail any of your questions regarding dental implantation!
Calculate the cost of treatment by taking a short test in 20 seconds!
Do not delay your treatment, because in this matter time plays against us.
The path of surgical dentistry to the development and full use of the method of direct implantation with immediate loading was one of the most difficult and lengthy in modern medicine. The study of the clinical and morphological features of the method, along with the development of new bone materials and implants, took decades.
One of the main reasons why the concept of immediate implantation justifies itself is the combination of the period of osseointegration with the healing of the tooth socket, stimulation of osseointegration, minimization of bone resorption and bone atrophy.
Theoretical foundations and
historical background
Branemark's discovery of the process of osseointegration, which occurred while studying the microstructure of the bone marrow, was the impetus for the introduction of dental implants into dentistry. The clinical application of this significant discovery was preceded by ten years of in vivo experimental studies to establish the degree of osseointegration of the implants and confirm the presence of direct bone-implant contact. The results obtained confirmed the absence of negative reactions from soft and hard tissues to the implants, which subsequently made it possible to begin clinical studies of dental implantation in humans.
As a result of the studies, the conditions necessary to ensure high-quality osseointegration of dental implants were determined. These include:
- Use of biocompatible materials.
- Compliance with the Bronemark protocol, which assumes a time period from implantation to loading on average of 3 to 6 months, as well as implantation into bone tissue that is completely healed after tooth extraction.
- Low tool rotation speed 900-1500 rpm when drilling bone.
- Using a buccal incision away from the alveolar ridge.
- Carrying out the procedure in a sterile hospital environment.
- Use only titanium tools and materials.
- No infectious process.
The variety of clinical situations and the need to accelerate the orthopedic rehabilitation of patients required a revision of the generally accepted Bronemark protocol, which was solved through the development of innovative methods of implantation, augmentation, the development of new models of implants, new osteoplastic materials and medical instruments, and the improvement of clinical diagnostics.
Currently, the two-stage Bronemark protocol remains frequently used, but the recommended atraumatic drilling to eliminate overheating of the bone tissue does not exclude osteonecrosis. The combination of mechanical damage and excess heat forms a devitalized zone of bone tissue up to 1 mm in size. It is known that heating the tissue near the drill to 38-41°C is sufficient for its death.
Due to the need for bone drilling, which will certainly lead to necrosis of the peri-implant area, it was advisable to propose minimizing the additional stress factor due to loading. This predetermines the holding period from the moment of installation of the dental implant to the load required for high-quality osseointegration, which does not reduce the relevance of the two-stage protocol today.
The use of modern tools and an individual treatment protocol in each individual case allows us to avoid and reduce the degree of undesirable results in the form of osteonecrosis. Prevention of osteonecrosis and fibrous encapsulation is achieved by modifying factors that lead to the formation of heat in bone tissue and are associated with the volume of preparation, the sharpness of drills, the depth of the osteotomy channel, etc.
It has now been proven that the phenomena of bone tissue necrosis can be minimized using the technique of preparing the osteotomy canal with a drill rotation speed of up to 1500 rpm and a drill cooling system. As a result of numerous improvements, the necessary primary stability of the implant was achieved within the limits of permissible micromotion, which led to the emergence and development of an innovative method of one-stage implantation.
Direct implantation with immediate loading has become possible in optimal clinical conditions, as well as with the appropriate size and design of the implant surface, the presence and sufficient volume of the required bone tissue biotype, the absence of additional stress factors and the infectious process. X-ray research methods are traditionally used to determine the clinical conditions for direct implantation.
First stage of the procedure: visualization of bone tissue
At the first stage of diagnostic imaging, as a rule, panoramic radiography is used, which allows one to obtain an image of the upper and lower jaw, the lower half of the maxillary sinuses. PR is far from the best diagnostic method in the context of obtaining detailed information, but it has a number of advantages.
The advantages of panoramic radiography include the ease of assessing the initial vertical height of the bone and macroanatomy of the jaws with the determination of existing major pathology, as well as the low cost and accessibility of the procedure for the patient. The disadvantages of PR are the lack of a detailed three-dimensional image of bone structures, as well as the inability to assess the quality of bone tissue and the degree of its mineralization.
Zoning using diagnostic templates is also not informative enough. Loss or repair of bone tissue from the vestibulo-oral side of the roots of teeth or an installed implant is not determined radiologically, since only the distal and medial areas are visible on X-ray films.
With the advent of computed tomography (CT), virtually all of the shortcomings associated with two-dimensional imaging of the PR have been eliminated. CT today represents a powerful digital method for obtaining three-dimensional images, allowing highly accurate diagnosis of the condition of tissues of different densities without the introduction of contrast agents. The technique reduces the risk of ongoing complications and relieves patients from psycho-emotional stress.
The use of an electronic version of three-dimensional images makes it possible to process data from one anatomical area on all CT sections with precise measurement of parameters and determination of the relationship between adjacent anatomical areas.
The role of the design, size and material of the dental implant
The possibility of effective direct implantation achieving osseointegration of titanium implants has been proven by histological studies in animals, as well as in humans. It was found that particularly careful consideration of implant size and design is required for the use of MNIN.
In the case of the two-stage Bronemark protocol, the length of the implant cannot solve the problems of reducing the load in the bone-implant zone, since the main load is concentrated in the edges of the alveolar process, namely its cortical layer. During direct implantation, the directed load affects the formation of the histological contact zone, so the length of the implant is important.
The resistance of implants is determined by different researchers relative to the average values of the plane of the roots of the teeth bearing the chewing load. Replacement of a tooth with an implant occurs according to the equivalent plane of intraosseous support. With MNINN and two-stage implantation, the width, length and design of the implant are important for the formation of bone-implant contact, since the main part of the stress from the mechanical load is concentrated at the edge of the bone
The length of the implant is important because it increases primary stability. This should also be facilitated by rational implant design. Remodeling and osseointegration do not occur simultaneously, so with a decrease in primary stability and simultaneous loading, there is a risk of exceeding the acceptable micromotion threshold, which will lead to implant loss.
Maintaining the micromotion threshold depends on bone type, implant surface treatment, and biomechanical load. The micromobility threshold, regardless of the surface coating of the product (for example, titanium implants with plasma spraying or bioactive implants) ranges from 50 to 150 μm.
For the direct implantation method with immediate loading, a screw implant with a maximum functional area is used, which is provided by the geometry, number and depth of the thread. The smaller the distance between the threads, the greater their number and the larger the surface area of the implant.
The thread depth also differs between designs. The greater the depth of the thread and the number of turns, the larger the supporting area of the implant. The use of implants of other shapes is ineffective for MNINN. It has been experimentally proven that there is no bone integration on the day of installation of a cylindrical implant with a tight fit, since there is no bone tissue between the threads.
The functional surface influences the rate of bone remodeling under occlusal loading. The geometry of the thread with a V-shaped and thrust profile determines the rate of early osseointegration of the bone-implant contact zone due to resistance to occlusal load forces, which reduces microstress in the bone tissue.
The condition of the implant surface ensures not only proper contact with bone tissue, but also a direct influence on the rate of osseointegration and the formation of distance or contact osteogenesis. The micro- and macrostructures of implant surfaces with different chemical structures have different effects on the stages of osseointegration.
Implant surface: rational choice
The use of a dental implant with a hydrophilic surface increases the adsorption of biological fluids with the subsequent attachment of blood plasma proteins at the stage of hemostasis, which accelerates osseointegration in the early stages. The presence of roughness or depressions of a certain size on the intraosseous part of the dental implant promotes the adsorption of proteins, mechanical retention of fibrin and collagen fibers, adhesion of osteogenic cells, and the synthesis of specific proteins and growth factors.
The relief allows you to significantly increase the specific area of the implant that interacts with the bone, which improves the quality of integration and reduces the level of mechanical stress of the surrounding bone tissue. The quality of the surface and its roughness is determined by the methods of processing the surfaces of the implants.
Below are the main types of surfaces used in the manufacture of dental implants for the direct implantation procedure with immediate loading.
SLA (andblasted with large grits and acid etched) is a surface that, as the abbreviation implies, is formed by coarse sandblasting followed by acid etching. Due to this type of processing, microdepressions measuring 2-4 microns in size appear on the surface of the product in the form of inclusions in the rough sandblasted surface.
Cell culture experiments, histological studies of bone, and animal experiments with implant removal indicate that SLA is a good choice for implant contact surfaces. In vivo studies have confirmed the superiority of SLA surfaces in implant integration and anchorage compared to other surfaces such as titanium plasma sprayed, machined or hydroxyapatite coated surfaces, especially during the initial healing phase after implant placement.
The most important property of the SLA surface, which plays a significant role in the development and practical use of implants, is the provision of a high load on it, which was confirmed experimentally in torsion experiments.
RBM (Resorbable Blast Media) is an implant surface created by sandblasting with beta-tricalcium phosphate particles of a certain density, mass and size. After mechanical processing, this surface is etched with a low-concentration organic acid, which makes the surface clean (without Ca3O8P2 residues), without modifying the structure of the titanium micropattern.
This method makes it possible to create micropores of greater depth on the surface of the implant than when treated with the traditional SLA method (aluminum oxide Al2O3). In this case, the surface area of the implant further increases due to an increase in the depth of the pores (craters), and its osteoconductivity increases accordingly.
Increasing the efficiency of osseointegration of implants with a bioactive coating also depends on the implantation technique and the patient’s bone tissue biotype.
Osseointegration of implants coated with hydroxyapatite occurs according to the principle of both contact and distant osteogenesis in certain peri-implant areas. With contact osteogenesis, new bone formation occurs directly on the surface of the implant itself.
The implementation of this mechanism occurs by analogy with osteoconduction. Hydroxyapatite on the surface of the implant acts as a passive matrix for osteogenesis. In this case, migration of progenitor cells occurs on the surface of the implant, which begin to differentiate into mature osteoblasts and secrete bone matrix on the surface of the implant under conditions of delayed loading.
Hydroxyapatite significantly reduces the rate of bone tissue remodeling under conditions of occlusal load, which has a positive effect on implantation results when applying immediate load in bone tissue biotype D4. In such situations, hydroxyapatite coating reduces the risk of overloading.
A comparative clinical and morphological assessment of implants with and without a bioactive coating one month after installation does not reveal any difference in the processes of osteogenesis.
Bone density as a factor in the success of dental implantation
Bone density is the most important factor for the success of dental implantation. According to the generally accepted international classification of bone tissue, there are four quality categories:
- D1 consists of homogeneous compact bone tissue.
- D2 bone consists of a thick cortex surrounding dense trabecular bone tissue.
- D3 bone consists of a thin cortex surrounding dense trabecular bone tissue.
- D4 consists of a thin cortex surrounding low-density trabecular bone tissue.
The likelihood of an implant not having micromobility and meeting the minimum required micromobility threshold directly depends on the bone tissue biotype. The lower the bone density, the lower the elasticity. The rate of remodeling of cortical bone tissue is much slower than trabecular bone tissue. In addition, differences in the preservation of lamellar structure are observed.
For one-stage implantation and MNINN, the ideal option is the presence of bone tissue of D1 biotype. A thick layer of homogeneous compact bone tissue is more often found in the anterior regions with a completely edentulous mandible. As the height of the alveolar ridge changes with a decrease in the volume of bone tissue, D1 is more often observed in the corresponding posterior parts of the mandible.
There is practically no implant mismatch for this biotype. The compressive strength of bone D1 is up to 22.5 MPa. In the practice of direct implantation with immediate loading, bone tissue with the full biotype D1 is not found, which is due to the environment of compacted, but trabecular bone tissue.
The preferred option for immediate loading is bone with biotype D2, let's say biotype D3 with a compressive strength of 7.5 MPa. Implant mismatch in biotype D2, namely the presence of cortical bone tissue of different densities and coarse trabecular tissue, is not predicted.
Clinical discrepancy is expected in bone biotype D4, in which there is thin cortical bone surrounding low-density trabecular tissue, and in some variants of biotype D3, in which thin cortical bone surrounds acceptable-density trabecular bone and has insufficient volume.
Taking into account the classification of bone tissue biotype and the corresponding localization by jaw sections when using INNNN can lead to a significant reduction in the risks of a negative result from a labor-intensive and expensive procedure.
Optimizing the load on dental implants
Currently, several approaches are proposed to reduce the occlusal stress factor of the load for direct implantation with immediate loading. In case of multiple missing teeth, a slightly larger number of implants are installed.
Some are loaded with a transitional prosthesis, others remain embedded in the jaws without loading during the normal bone healing period. After the period required for osseointegration, the preserved implants, loaded during the specified period, are also included in the orthopedic design.
Another protocol involves immersion of all installed implants from the very beginning, with the possible placement of additional structures in the bone-implant contact areas to reduce stress. Immediate loading with partial absence of teeth, including the loss of single teeth, was carried out taking into account the possibilities of their unloading, which was achieved by removing the orthopedic structure from occlusal contact.
The necessary conditions for successful dental implantation, related to a sufficient amount of surrounding bone tissue and the shape of the implant, are listed below:
- All alveolar walls must be preserved and have a thickness of at least 2 mm.
- Below the bottom of the socket of the extracted tooth there must be at least 3-4 mm of bone tissue to ensure reliable primary fixation of the implant.
- The implant must match the length and diameter of the socket as accurately as possible.
These conditions were partially achieved using additional modern techniques, instruments for traumatic tooth extraction and implant installation, and the use of osteoplastic materials. Atraumatic tooth extraction with one-stage implantation is of great importance for the success of osseointegration.
The discrepancy between the shape of the tooth socket and the shape of the implant, the loss of one or more walls of the socket negatively affects the result of the procedure. It is necessary to have three or four alveolar walls for successful implantation. Achieving primary implant stability in the absence of two or more alveolar walls is unlikely, even despite the seemingly sufficient bone reserve.
The availability of modern instruments and the emergence of new methods of tooth extraction using ultrasound makes it possible to successfully carry out atraumatic removal. In the past, the presence of inflammation in the tissues surrounding the tooth socket and the alveolar bone adjacent to the implant bed was considered an absolute contraindication to the procedure. Thanks to the experience of successful osseointegration of implants when installed in an infected tooth socket under the cover of antibacterial anti-inflammatory therapy, this contraindication has become relative, that is, according to modern concepts, it is not necessary to maintain absolute sterility of the surgical wound.
In cases where the shape of the socket coincides with the shape of the implant, the design features of modern implants with their gum formers make it possible to form the contour of the mucous membrane of the cervical area and prevent its growth into the implantation zone.
Use of dental membranes
In the vast majority of situations, there is a need to use osteoplastic materials and special methods for treating soft tissues. The lack of immune protection in the area of osteoplastic material before the onset of active angiogenesis with the final formation of the microvasculature requires measures to prevent peri-implantitis.
If microorganisms enter the peri-implant area, the bone material becomes an excellent substrate for bacterial growth, which quickly leads to disruption of osseointegration processes and loss of the implant. To prevent infection of the surgical field, insulating membranes made from modified biocomposite osteoplastic materials are used and have antimicrobial properties and antibacterial drugs in the postoperative period.
High-quality osseointegration of the implant occurs with complete overlap and subsequent preservation of the mucous-oxide flap or simply the presence of mucous membrane over the implant while maintaining all the walls and sufficient thickness of the alveolar process. High-quality osseointegration does not occur in areas with a significant deficiency of bone tissue (more than 1.5 mm), especially in the cervical area, with fenestrations or a significant fracture of the vestibular wall of the alveolus due to unsuccessful extraction.
Prevention of epithelial growth in the implantation zone, as well as isolation of osteoplastic materials from the negative effects of oral microflora, became possible only with the advent of biological membranes. The following types of membranes are distinguished:
- Non-resorbable membranes. Using non-resorbable membranes, bone tissue defects larger than 3 mm are restored. This type of membrane allows you to restore bone tissue within clearly defined boundaries. Having a rigid fixation contour, frame titanium membranes prevent collapse in the intervention site, thereby making it possible to restore bone tissue both vertically and horizontally in large volumes.
- Resorbable membranes include natural ones (collagen and laminated demineralized lyophilized bone), as well as certain synthetic ones (calcium sulfate, polymers). In the case of using the direct implantation technique, the use of resorbable membranes is more justified, since this technique produces the maximum possible atraumatic tooth extraction while maintaining the contour of the hole in the cervical area with a given height.
Special methods of tissue processing using osteoplastic materials are necessary for direct implantation with immediate loading. The spread of directed tissue regeneration made it possible to prevent not only the premature growth of epithelium into the surgical wound, but also the augmentation of the alveolar ridge. Modern advances in mucogingival surgery (techniques using pedicled flaps, island flaps) make it possible to ensure tissue regeneration.
Bone materials for direct implantation with immediate loading
General and local factors leading to progressive resorption of the jaws have necessitated the development of tissue transplantation and biomaterial science. The development of measures aimed at replacing bone defects in the human body, including the maxillofacial area, has led to the introduction of a number of bone grafting methods into dental practice.
These methods include the following:
- Autogenous transplantation, in which the transplantation of organic bone material occurs within the same organism.
- Allogeneic transplantation, in which the transplantation of organic material occurs from a genetically related organism (from person to person).
- Alloplasty, in which the replacement of bone defects is performed using materials of inorganic origin.
- Xenogeneic transplantation, in which organic material is transplanted from a genetically unrelated organism (animal origin, mainly cattle).
The use of osteoplastic materials for direct implantation with immediate loading has some features that will be discussed in more detail below, taking into account their capabilities and limitations.
Autogenous bone
The gold standard is the use of autologous bone, when the donor and recipient are genetically identical. Autogenous bone is the only material that immediately has the necessary osteogenic, osteoinductive and osteoconductive properties.
Osteogenic properties are inherent in grafts containing living cells that grow into the recipient site and stimulate the growth of new bone. Osteoconduction is the ability of a material to play the role of a passive matrix for new bone, that is, to serve as the basis for the maturation of bone tissue present in the defect. The listed characteristics are determined by the surface structure of the materials.
The osteoinductive properties of osteoplastic materials are manifested in the presence of morphogenetic proteins in them, which induce differentiation of mesenchymal cells from osteoblasts in the bed. This whole “triad of success”, osteogenicity, osteoconductivity and osteoinductivity, is characteristic exclusively of autologous bone.
Autogenous material is collected from both intra- and extraoral areas. When taking intraoral material, the ideal site is the mental triangle due to easy access and the presence of a thick layer of cortical bone containing more morphogenetic proteins than cancellous bone.
In the oral cavity, biomaterial is collected within the hill of the upper jaw and lower jaw in the area of the ramus and chin. From extraoral sites, long tubular bones are rarely used for collecting material; relatively often, the ilium is used.
The main disadvantage of using autogenous transplants is the need for additional surgical interventions, leading to injuries and psycho-emotional stress for the patient.
Allogeneic transplants
Allogeneic bone materials are also produced from human bone, but the donor and recipient differ in genetic aspects. This material can exist in mineralized and demineralized forms. Demineralized bone also exhibits osteoinductive properties due to easily diffusible proteins.
Despite all the advances in immunological and genetic diagnostics, cases of transmission of infectious diseases such as Creutzfeldt-Jakob disease, HIV and hepatitis C with bone tissue are still recorded. Low efficiency of using fresh allogeneic bone, the risk of transmission of infections, as well as the prohibition of the church in some regions of the world were forced to abandon such transplantation.
Despite these difficulties, cadaveric bone, after appropriate processing, is now widely used in domestic dentistry.
Alloplastic materials
Alloplastic materials include numerous synthetic products (hydroxyapatite, tricalcium phosphate, bioactive glass) or plant products of organic origin (seaweed, corals).
These materials are biocompatible, antigen-inactive, non-carcinogenic, also do not cause inflammatory reactions, are radiopaque, can be sterilized without loss of properties, and are resistant to high temperatures and humidity. They have only osteoconductive properties.
Xenogeneic bone materials
The appearance of xenogeneic materials after the experiments of Ollier, who transplanted bone fragments between different biological species, occurs in the second half of the 19th century.
Xenogeneic transplants are obtained from animals, so the donor and recipient are foreign in appearance. The main source of xenogeneic materials is cattle bones (Osteomatrix, Bio-Oss, Cerabone). Sometimes pork bones (OsteoBiol-MP3, The Graft) or horse bones (Bioteck) are also used.
There is a pattern: if bone tissue taken from animals belonging to a primitive species is transplanted into animals with a higher level of organization, the results are much better and more predictable than when bones are transplanted from highly organized animals to lowly organized ones.
The resorption time of these materials is also different. Resorption of material with simultaneous physiological replacement by bone tissue is a necessary phenomenon during implantation. But for some materials, complete resorption does not occur. It has been established that they remain included in the newly formed bone matrix.
After the advent of modern methods of production and sterilization, xenogeneic bone materials are widely used in dentistry, including the method of direct implantation with immediate loading. The presence of pronounced osteoconductive properties of xenogeneic materials has determined their advantage over other osteoplastic materials and made them the material of choice after autograft. Sufficient quantity, availability and safety also contribute to their use in surgical practice.
Role of sulfated GAGs
The method of preparation, micropore size, resorption time and properties of the above materials may vary significantly depending on the specific manufacturer and its product. Advanced domestic bone materials, such as Osteomatrix, have osteoinductive properties due to the presence of sGAG, or sulfated glycosaminoglycans.
Sulfated GAGs are an important component of the extracellular matrix. In the periodontium, they are located in the walls of blood vessels and along the entire periodontal membrane. Their content is especially increased in the area of the circular ligament of the tooth.
It has been established that the synthesis of sulfated GAGs always precedes the synthesis of collagen. Thus, when an additional amount of GAG is introduced, the cell immediately has the opportunity to begin the synthesis of collagen, which accelerates the repair process.
Sulfated glycosaminoglycans interact with collagen molecules and affect the formation of collagen fibers, which promote the laying of tropocollagen molecules in fibrils, and fibrils in fibers, while simultaneously limiting their growth in thickness. sGAGs stimulate angiogenesis, accumulate and release growth factors, bind calcium and control the mineralization of the organic bone matrix.
It has also been established that one hundred sGAGs have an anti-inflammatory effect due to the inhibition of enzymes that destroy the intercellular matrix and the biosynthesis of inflammatory mediators. sGAGs additionally support free radical inhibition. Recent studies have confirmed that sGAGs have an anti-edematous effect, which is ensured by the fact that GAG chains, due to their hydrophilicity, adsorb moisture, significantly reducing the swelling of surrounding tissues.
In addition, these bioactive molecules induce osteogenesis, which occurs by creating optimal conditions for the proliferation and differentiation of osteogenic cells and enhancing the action of growth factors.
Advantages of direct implantation with immediate loading
According to observations, during the first year after tooth loss, the width of the alveolar process bone decreases by 25%, and the total height loss is up to 4 mm. Long-term studies of edentulous patients over 25 years using lateral cephalograms demonstrate persistent bone loss. In this case, atrophy of the lower jaw bone can be 4 times greater.
According to Wolff's law, bone requires constant stimulation to maintain its shape and density and undergoes remodeling depending on the forces applied to the tissue. The parameters of the internal architectonics and external configuration potentially change with modification of this impact. The consequence of tooth loss with a corresponding decrease in bone stimulation results in a decrease in bone density and width.
Mechanical support and preservation of bone tissue in contact with the implant occurs subject to the physical presence of the implant. Taking into account the stress effects on the bone during the immersion of implants during direct implantation, the key determining factor in the success of treatment is the type of bone tissue.
Clinical studies on the survival of implants with identical designs and standard surgical protocols have not found the same results for all types of bone density. The density of the alveolar bone, as a consequence of the mechanical deformation that occurs during microstress, is significantly higher at the ridges around the teeth than in the periapical region.
Loss of bone density occurs not only after tooth loss, but also in the absence of occlusal load. Bone density will be higher if there is a root in the tooth socket, even without occlusal load.
Precise selection of an implant into the socket of an extracted tooth, the perimeter of which has denser bone tissue, improves primary stabilization regardless of the bone tissue biotype. Immediately after tooth extraction, there is a massive movement of cells with high osteogenic potential into the alveolus, coming from the exposed bone marrow spaces of the jaw and periodontal ligament.
If the tooth is in a normal position in the dentition, installation of the implant does not cause any difficulties, since it is placed along the extracted root in the socket, and the reduction in the invasiveness of bone drilling prevents overheating.
In addition to the clinical aspects of dental implantation, there is also a psychological aspect. Traditional fixed prosthetics has a negative impact on patients due to the need to prepare teeth adjacent to the defect.
Treatment according to a two-stage protocol involves the use of temporary orthopedic structures, causing discomfort when eating, talking or other everyday situations. In addition, with this type of implantation, complications are possible in the form of deterioration of osseointegration and reduced aesthetics of the implant-supported orthopedic structure.
An important advantage of direct implantation with immediate loading compared to other methods is the reduction of the psycho-emotional burden on the patient due to a reduction in the number of surgical interventions and the provision of the ability to quickly replace a tooth with an implant. Most patients accept an implant-supported prosthesis as an integral part of their own body.
Thus, using existing methods for installing implants, special tools, materials and auxiliary techniques, it is possible to create all the necessary conditions for high-quality and safe direct implantation with immediate loading, from tooth extraction to the installation of orthopedic structures.
Cost of implantation with immediate loading
Since implantation with immediate loading is a one-stage implantation that involves fewer manipulations, it will have a lower cost compared to classical dental implantation. However, the exact price of implantation with immediate loading can only be found out in the clinic and here’s why:
- You need to decide on the implantation technique;
- Select implants;
- Consider the cost of preparatory procedures and temporary prosthesis.
And if you are interested in the price of turnkey implantation, then you need to take into account in the total cost the price of a permanent prosthesis, which can be made from different materials and using different technologies. Therefore, to determine your possible costs for dental implantation, the best thing to do is come to the clinic and ask the implantologist to create an individual treatment plan for you!
Examples of work “Before” and “After”
Complex one-stage implantation of the lower jaw
Case: there was a loose bridge of 4 front teeth on the lower jaw; after diagnosis, removal of the remaining teeth and complex basal implantation were prescribed.
Dental restoration using basal implantation method
Case: complete absence of teeth in the upper jaw, bone atrophy.
Restoration of all teeth using basal implantation method (March 2012)
Case: partial adentia, exposed roots of natural teeth, periodontitis, increased tooth mobility, severe atrophy of bone tissue in some places beyond the possible norms for classical dental implantation.
Restoration of anterior teeth using basal implantation method (April 2012)
Case: partial absence of front teeth and destruction of supporting teeth under the prosthesis, the relief of the gums and interdental papillae is disturbed.