Giuseppe Cantatore University of Verona (Italy). Department of Endodontics. Assistant professor.
In a classic study published in 1985, Bystrom et al. compared the sterilizing effectiveness of three different methods of endodontic treatment of infected canals and found that mechanical treatment in combination with irrigation with saline solution ensures canal sterility in 20% of cases, while replacing NaCl with a 5% sodium hypochlorite solution leads to canal sterility in 50% of cases. cases, and the addition of the latter scheme with a single temporary filling of the canal with calcium hydroxide increases the percentage of canal sterilization to 97%. Does this mean that when treating infected root canals, temporary filling with medicated paste is required in all cases? More than 15 years have passed since the Bystrom et Al study; Today we know much more about the properties of microorganisms associated with pulp-periodontal pathology: from virulence to mobility, from the ability to penetrate dentinal tubules to sensitivity to various antiseptics. 15 years of research experience have shown that many irrigation solutions have pronounced bactericidal activity against microorganisms such as enterococcus faecalis or candida, which are resistant to calcium hydroxide or chlorophenol. In this article, we will discuss in 7 points how to improve the root canal irrigation procedure, using the right products in the right sequence, in order to reduce the need for additional medicinal treatment of the canals between visits.
Key Factors for Effective Cleaning and Irrigation of the Root Canal System
1. Thorough diagnosis of existing pulp-periodontal pathology
2. Taking into account the condition of the tooth tissues and the complexity of the anatomy of the root canal system3. Removal of the endodontic smear layer4. Compliance with indications when choosing irrigation products5. Optimization of the active components of the irrigation solution6. Correct sequence of application of irrigant solution during root canal treatment7. Mandatory costs of at least 5 minutes for irrigation before filling
Dental clinic No. 2
Analysis of the reasons for the failure of endodontic treatment led to some rethinking of the meaning of its individual stages. Biological prerequisites, such as the complexity of the internal morphology of the tooth, as well as intracanal biofilm, force the search for new effective methods for cleaning root canals. And in this regard, the problem of high-quality root canal irrigation as the key to successful endodontics comes to the fore. The article provides a classification and brief description of the main irrigation techniques in endodontics, and provides practical recommendations for the use of the most popular of them.
If we analyze the scientific endodontic literature over the past few years, it becomes quite obvious that in the process of endodontic treatment, the irrigation phase is given great importance. Cleaning the root canal system of pulp residues, microorganisms and their toxins is a key point in treatment, without which it is impossible to hope for a successful result. The beginning of the clinical use of rotating N&T instruments was accompanied by a certain “euphoria” due to the “virtually unlimited capabilities” of these instruments. Indeed, most studies indicate a significant difference in the quality of root canal preparations performed with hand instruments and rotating N&T systems. However, the use of modern research methods, such as electron microscopy, computed microtomography, microbiological tests, etc., has shown that it is not possible to qualitatively clean the root canal system only through mechanical removal of infected dentin and pulp residues with manual or machine endodontic instruments possible.
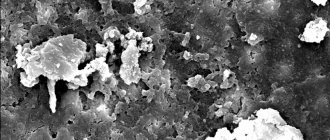
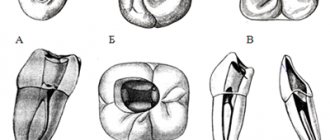
Today, endodontic science has extensive information about the structure of the root canal system. It is known that the internal morphology of the tooth is extremely complex and diverse. A perfectly round cross-section, tapered root canal with a single apical foramen is perhaps the rare exception and not the rule. In the vast majority of cases, the canals have an irregular shape, different diameters in the buccolingual and mesiodistal directions, and numerous undercuts, the so-called “fins” (photos 1, 2). Oval or shaped canals are often found. In addition, many lateral tubules arise from the main canal at different levels. Lateral tubules are also found in the area of bifurcations and trifurcations of multi-rooted teeth. There are numerous anastomoses and isthmuses between the root canals, which are especially common, for example, between the medial canals of mandibular molars. The morphology of the apical third of the root is very complex. It is known that the main canal in the apical part forms a delta and opens at the root apex with not one, but several apical openings. Based on the above, it becomes obvious that such a complex system is not possible to clean only mechanically. In this regard, high-quality and effective irrigation of root canals becomes of great importance. Another major problem in root canal disinfection is intracanal biofilm. Its role in the prognosis of endodontic treatment is difficult to overestimate. According to the modern concept, microorganisms in root canals are present in the form of a bacterial biofilm, which significantly changes their properties and makes it difficult to eliminate them from the root canal system. Biofilm is a community of microorganisms surrounded by an extracellular polysaccharide matrix and attached to a moist surface. The biofilm protects the microorganisms present in it from the effects of adverse factors, creates conditions for reproduction; the polysaccharide matrix prevents the penetration of antibacterial agents into the biofilm, thereby increasing the resistance of microbes to antiseptics and antibiotics. Therefore, to eliminate biofilm, a combination of both a mechanical factor that can destroy the structure of the biofilm and a disinfectant that destroys its constituent microorganisms is necessary.
Thus, irrigation has two important goals:
cleansing the root canal system due to the chemical dissolution of organic and inorganic residues, as well as their mechanical washing out with a stream of liquid; disinfection of the root canal system.
In this regard, cleaning the root canal system should be considered as the most important stage of endodontic treatment, which has a significant impact on its prognosis. In turn, high-quality preparation and formation of the root canal helps create the necessary reservoir for the irrigation solution and opportunities for its activation.
All irrigation techniques can be divided into 5 groups:
manual; ultrasonic; sound (EndoActivator); laser (the solution is activated by a laser); hydrodynamic (RinsEndo, Endo Vac).
Manual irrigation
Traditional methods of irrigation using a syringe and endodontic needle provide satisfactory treatment of the coronal and middle third of the root canal, but are not sufficiently effective in terms of cleaning its walls in the apex area. For successful irrigation, it is necessary that the disinfectant solution be delivered to the entire working length of the root canal. This is not always possible to achieve with the help of classic endodontic syringes and needles, since in narrow root canals, due to surface tension, the irrigation solution does not reach the apex, leaving a so-called “air bubble”. As a result, the apical part of the root canal remains insufficiently processed. There are a number of simple rules and techniques that can make syringe irrigation more effective and predictable. The effectiveness of this type of irrigation is limited to a distance of 3-4 mm from the tip of the needle. Consequently, the closer the needle is advanced to the apex, the higher the quality of canal cleaning. On the other hand, the likelihood of the irrigation solution being carried beyond the apex also increases. In order to prevent this complication, it is very important to have some distance between the tip of the needle and the wall of the root canal (Fig. 1a, b). The next important points are the movements of the needle during the introduction of the irrigation solution, as well as the position of the syringe. The irrigation solution should be withdrawn slowly and carefully, while the needle should make reciprocating movements. It is recommended to press on the syringe piston with the index finger rather than the thumb, as tactile control is significantly improved (photo 3a, b).
The depth of needle penetration, in turn, is determined by the following factors:
the size of the apical preparation; channel taper; needle diameter.
The optimal size of the apical preparation for effective irrigation should be 30-40 according to ISO.6 The relationship between the apical size and taper can be schematically represented as follows (Fig. 2).
After completing the preparation of the canal with a hand file No. 25 (taper 2%), it can be assumed that its diameter at a distance of 3 mm from the apex will be 0.31 mm (0.25 + 0.02x3).
When using a rotating nickel-titanium instrument with the same tip size, but a 6% taper, the channel diameter at the same level will already be 0.43 mm (0.25 + 0.06x3).
At a distance of 10 mm from the apex, the difference will be even more significant - 0.45 and 0.85 mm, respectively. Thus, a pronounced taper significantly improves the efficiency of irrigation, creating an additional depot for the solution and allowing it to act throughout the canal (Fig. 3). The next important factor is the diameter of the needle. The diameter of needles is usually measured in units called gauge. The most commonly used endodontic needles are 27 gauge. It should be remembered that when determining the size of needles, an inverse relationship is observed. The larger the number in gauge, the smaller the needle diameter (Table 1). Thin needles Endo-Eze Tips and NaviTip (Ultradent) have a diameter of 29 gauge (0.28 mm), which allows them to be advanced as much as possible to the apex (photo 4).
A very important characteristic is the flexibility of the needle and the ability to pre-bend it when working in a canal with pronounced curvature.
To increase the effectiveness of manual (performed with a syringe) irrigation, a gutta-percha pin can be used, which is used to mechanically activate the irrigant in the pulp cavity and root canals9 (photo 5a, b). Company
Ultradent offers the NeviTip EfX endodontic attachment, which is both a needle and a brush for mechanical activation of the solution. Using NeviTip Effect, you can simultaneously carry out the stage of irrigation and mechanical cleaning of the canal from sawdust, old filling material or calcium hydroxide (photo 6, 7).
Ultrasonic irrigation
A very effective method of activating an irrigation solution is the use of passive ultrasonication. With passive ultrasonic irrigation, a thin wire or a small file, for example No. 15 or 20, is inserted into the root canal filled with solution (photo 8). Ultrasonic vibrations and the energy of the file are transferred to the liquid, which causes the occurrence of so-called acoustic cavitation. At the moment of rarefaction, cavitation bubbles appear in an intense sound wave, which collapse sharply when moving to an area of high pressure. In the cavitation region, powerful hydrodynamic micro-shock waves and micro-flows arise. In addition, the collapse of bubbles is accompanied by strong local heating of the liquid and the release of gas. Such exposure leads to the destruction of even such durable substances as steel and quartz. If sodium hypochlorite is used as a solution during passive ultrasonic irrigation, its antibacterial effect is significantly enhanced. In addition, local temperature increases also play an important role. Thanks to these effects, dentinal filings, pulp tissue and intracanal biofilm are removed (including due to the dissolving effect of NaOCl). In order to remove this suspension from the canal, you need 2 ml of fresh solution, which is injected from a syringe.
Practical recommendations for performing ultrasonic irrigation:
the size of the ultrasound file should not be more than 15, 20 according to ISO; the files used should not have a cutting surface to prevent transport of the canal (photo 9); the file should be inserted into the canal, 1.52 mm short of reaching the working length (photo 10); it is important to limit the reciprocating movements of the instrument in the canal and always pre-bend the file when working in curved root canals in order to prevent apical perforation and the formation of steps; the solution is sounded 3 times for 20 seconds, with the obligatory renewal of the irrigant in a volume of 1.5-2 ml.
Sonic irrigation
In addition to ultrasonic energy, sound vibrations are also used to activate the irrigant solution in the root canal. Compared to ultrasonic devices, sound devices generate vibrations of lower frequency but higher amplitude. As a result, the point contact of the sonic tip with the wall of the root canal does not actually affect the effectiveness of its work - unlike ultrasonic tips. A number of researchers have shown that sonic activation of the solution improves the quality of root canal irrigation compared to manual techniques. An example of a sound system for use in endodontics is the Endo Activator (Advanced Endodontics). An interesting design feature of this system is that it uses special polymer tips that do not have cutting properties and, therefore, avoid complications such as the formation of a step, transportation, and perforation of the root canal walls. In addition, the tips are disposable and can be easily selected and trimmed depending on the length and diameter of the root canal. On the other hand, the quality of treatment of the apical part of root canals using sound activation is still significantly inferior to that using passive ultrasonization.
Hydrodynamic irrigation
To improve the quality of treatment of the apical third of the root, the RinsEndo system from Duerr Dental (RinsEndo, Durr Dental, Germany) was also developed. RinsEndo is a handpiece that screws onto the turbine drive of the dental unit and uses compressed air pressure to propel the irrigant solution into the apical part of the root canal. A study conducted by W. Hauser et al demonstrated the high efficiency of cleaning the root canal walls with this system compared to traditional manual syringes. But at the same time, this work showed that the use of the RinsEndo tip significantly increases the likelihood of the irrigation solution being removed beyond the apex (80% versus 13% when using a conventional syringe), which is especially dangerous when using sodium hypochlorite solution as an irrigant due to the possibility of serious complications. Another option for solving the problem of insufficient cleaning of the apical third of the root canal is the use of systems based on creating negative pressure in the canal. An example of such a system is EndoVac from Discus Dental. The basis of traditional irrigation methods is the passive introduction of an irrigant solution into the root canal under the influence of positive pressure applied to the syringe plunger. The principle of operation of the Endo Vac system is based on the movement of the irrigation solution by creating negative pressure in the root canal. One of the nozzles, which supplies the irrigation solution, is inserted into the tooth cavity to a shallow depth, while the other cannula, which performs aspiration, is inserted into the root canal to its entire working length. As a result, the supplied solution, due to negative pressure, penetrates the entire working length of the root canal without the risk of being carried beyond the apex. The advantages of this technique compared to the traditional irrigation method have been confirmed by a number of scientific studies.
Activation of irrigant by laser radiation
A relatively new and interesting trend in root canal irrigation is photoactivated disinfection (PAD or PDT). The essence of the method is the introduction of a special dye - a photosensitizer - into the root canal, followed by irradiation using low-power laser radiation with a certain wavelength. Light-sensitive dye molecules (the most commonly used dye is tolonium chloride, or TBO) attach to or even penetrate the bacterial cell membrane. Then, under the influence of laser radiation with a certain wavelength (for tolonium chloride it is 633 nm), a chain of chemical reactions is launched, which results in the formation of free radicals, namely singlet oxygen. These active radicals cause disruption of the integrity of the bacterial cell wall, inactivation of bacterial toxins, degradation of essential proteins and DNA molecules, resulting in the death of the bacterial cell.8 The high antibacterial activity of photoactivated disinfection against both suspended cultures and bacterial biofilm has been demonstrated in a number of studies . The key point of this technique is the direct contact of photosensitizer molecules with the bacterial cell and its penetration into the bacterial biofilm. Consequently, as in the case of the use of traditional irrigation methods, the problem of delivering irrigant (dye) to hard-to-reach corners of the root canal system remains relevant.
Conclusion
In conclusion, I would like to note once again that today the endodontic treatment strategy is increasingly inclined to use the concept of the biological feasibility of the intervention. This approach, in turn, led to the need to improve methods of combating intracanal biofilm as the main reason for the failure of endodontic treatment. And the key point in this fight is high-quality irrigation of the root canal system.