Root canal filling – this method is used in dentistry in the treatment of dental diseases such as pulpitis or periodontitis. Before filling the canals, they are always subjected to antiseptic and mechanical instrumentation. The latter allows you to expand the lumen of the root canals and make their walls smoother - without which their high-quality filling is simply impossible. Filling of the canals is carried out using radiopaque materials so that the doctor can evaluate the quality of treatment using radiographs.
Most often, gutta-percha pins are used for this in combination with a special sealer (paste). Only a high-quality filling can prevent the subsequent proliferation of infection in the root canals, as well as at the apex of the tooth root. And well-filled root canals of teeth must meet a number of criteria, which we will discuss in this article. We will also talk about the main mistakes dentists make, each of which we will demonstrate to you on targeted X-rays.
Important: at the moment (according to official statistics) filling of root canals in the treatment of pulpitis and periodontitis in 60-70% of cases is performed poorly by dentists. This subsequently leads to the development of inflammatory complications and even tooth extraction - in the short and long term, respectively. Retreatment of such teeth is very expensive, because... associated with the need for their preliminary unsealing, after which they are re-sealed.
Dentists' mistakes when filling canals -
- Incorrect measurement of root canal length –
Root canals in a tooth must be filled strictly to the apex of the tooth root.
To do this, it is necessary to correctly determine the length of each root canal. Errors at this stage lead to the fact that the canals are either filled not to the apex of the root, or the filling material is carried beyond the apex of the root, directly into the bone. In the unfilled part of the canal, an infection develops, which leads to the formation of inflammatory foci at the apexes of the roots of the teeth, for example, apical granulomas or radicular cysts, which is accompanied by periodic suppuration and the appearance of pain when biting on this tooth. Refilling the canals can also lead to long-term pain, neuralgia, numbness of the lip and chin.
- Poor quality mechanical processing of the canals - such processing is necessary to widen the canals and give them a slightly conical shape. Only under this condition can they be sealed later. Numerous mistakes by the dentist at this stage (insufficient expansion of canals, formation of steps, root perforations) lead to subsequent poor-quality fillings and, again, to the development of inflammatory complications requiring new expensive retreatment.
Upper second molar
Upper second molar.
Usually this tooth is a small replica of the first molar, but the roots usually diverge less and the fusion of the two roots is more common. The predominant form is with three canals and three apical openings, the average length is 21 mm.
Fusion of roots is found in 45-55% of Caucasians, and Mongoloids in 65 to 85% of cases. In these cases, usually the mouths of the canals and they themselves are located closer to each other or merge.
Access contours in the upper molar.
Stages of root canal treatment –
High-quality filling of root canals in the treatment of pulpitis and periodontitis is the key to the absence of complications. But in order to fill the root canals, they must first be prepared for this. Since the root canals are very narrow, preparation for filling will consist of widening the canals and extending them along their entire length to the apex of the root.
Let's imagine that there is a deep carious cavity on the chewing surface of the tooth, and the tooth pulp is inflamed.
The main stages of root canal filling are:
- Removal of all tissues affected by caries (Fig. 2) - in this case, healthy tooth tissues can also be partially removed in order to create convenient access to the mouths of the root canals.
- Removal of dental pulp – pulp is removed from both the coronal part and the root canals.
- Determining the length of each root canal - each canal has its own length and depends on the length of the root and bends.
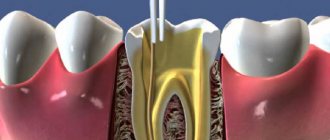
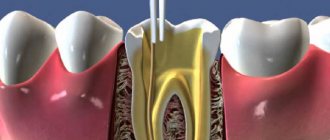
- Mechanical treatment of root canals (Fig. 3) - it is necessary to use special tools to go through the root canals the entire length to the apex of the root, and then expand the diameter of the canals to the desired size. If this is not done, it will not be possible to qualitatively seal the canal along its entire length (especially its far third at the apex of the root).
- Filling canals with gutta-percha (Fig. 4) is the final stage of working with root canals. The quality of this stage directly depends, first of all, on the correct measurement of the length of the root canals and on the quality of their mechanical processing.
Lower central and lateral incisors
Lower first incisor. (I channel configuration type).
Both teeth have an average length of 21 mm, although the central incisor is slightly shorter than the lateral incisor. The morphology of dental canals can have one of three configurations.
Lower second incisor. (IV channel configuration type).
Type I - one main canal from the pulp chamber to the apical foramen.
Type II/III - two main canals that merge in the middle or apical third into one canal with one apical foramen.
Type IV - the two main canals remain separate for the entire length of the root and with two apical foramina.
All studies show that type I is the most predominant. Two channels are recorded in 41.4% of cases, and type IV - in 5.5% of cases.
There is evidence that in Mongoloids, two canals are less common in these teeth.
The pulp chamber is a small replica of the upper incisors. There are three pulp horns, not very well defined, and the chamber is wider in the labial-lingual direction. In the version with one channel, it can bend towards the distal and, less commonly, towards the labial side. The canal begins to narrow in the middle third of the root and becomes round. With age, the changes are the same as in the upper incisors and the pulp chamber can be located below the level of the neck of the tooth.
The main stages on which the quality of root canal filling depends:
1) Determination of the working length of each root canal -
High-quality root canal treatment requires that the root canals be filled to the apex of the root. If the channel length is determined incorrectly, then there are 2 options :
- The root canal will be underfilled - this will lead to inflammatory complications, the development of periodontitis, cysts, and in the absence of retreatment of the tooth - to its removal.
- The root canal will be refilled - the filling material will be excessively removed beyond the apex of the root, and this can lead to long-term pain, neuralgia, and the development of inflammation.
Therefore, it is necessary to carefully measure the length of each canal in the tooth. This is done in good clinics as follows: after removing the pulp from the root canals, the doctor, using special thin hand instruments (for example, K-files - Fig. 7, 10) tries to go through each root canal to the apex.
The advancement of the instrument deep into the canal is carried out under the control of a special device “apex locator” (Fig. 6), which is connected with the help of an electrode to the K-file located in the canal (Fig. 7-8). The display of the apex locator reflects the depth of the instrument's immersion, as well as the moment the instrument tip reaches the root apex.
Important: the apex locator only shows an approximately accurate picture. Therefore, after measuring the length of the canal with an apex locator, the K-file is left in the root canal and the patient is sent for an x-ray. These K-files are radiopaque, so the X-ray can clearly see whether the tip of the instrument has reached the apex of the root.
2) Mechanical treatment of root canals –
The purpose of mechanical treatment is to expand the root canal and make it suitable for filling.
Untreated canals in most cases are very narrow, have many imperceptible narrowings and expansions, which will not allow the canal to be properly filled with filling material along its entire length. Thus, mechanical treatment should remove all narrowings and irregularities throughout the root canal, and expand it to a certain size.
There are 2 methods of mechanical treatment of root canals:
- Hand instruments (Fig. 10) - the doctor rotates such instruments in the root canal with his fingertips. Below you can see photos and videos of this method.
- Using an endodontic tip (Fig. 11) - special Pro-files made of nickel-titanium are inserted into such tips (Fig. 12). The endodontic tip rotates the profile in the root canal, as a result of which the sharp edges of the profile remove chips from the walls of the canal, expanding it. Due to the fact that the metal of the profiles has a shape memory effect, they do not break during rotation even in highly curved root canals.
The advantages of processing canals with such machine Pro-files over hand tools:
- The quality of canal treatment is many times higher - the surface of the root canal walls after such treatment is very smooth, as if polished, and this facilitates the insertion of gutta-percha pins for filling the canal. In addition, the use of an endodontic tip can significantly reduce the processing time of canals (compared to manual processing).
- Safety - in most cases, the endodontic handpiece comes complete with a smart micromotor (Fig. 11), which controls the movement of the file in the canal.
If a certain load is exceeded, which threatens to break the profile in the channel, the micromotor stops the rotation of the profile and turns on auto reverse. Therefore, the threat of the tool tip breaking off in this case is minimal, which cannot be said about manual files. After all, the doctor’s fingers, with which he rotates the “manual” file, feel quite weakly the extreme resistance to the movement of the instrument, after which the instrument breaks off in the canal. If your clinic performs mechanical treatment of canals using such smart devices, this is a big plus. However, it is worth remembering that in any case such treatment is performed by a doctor, and even the smartest and best device in the wrong hands can cause more harm than good (24stoma.ru).
Mechanical treatment of canals with hand instruments and endodontic handpiece: video
3) Filling root canals with gutta-percha –
After the root canals have been expanded and the root canals have been treated with medication, they need to be sealed. Root canal filling methods that can be used in dental clinics:
- One paste method - the canal lumen is filled with a plastic material, which then hardens. At the moment, there is no more terrible method of filling canals; complications develop in almost 99% of cases. If your doctor fills your canals in this way, then you need to run urgently! And if you can’t run, then you should at least crawl to the exit.
- Single pin method - after filling the root canal with paste (as in the previous version), one gutta-percha pin is inserted into the root canal. This method is slightly better than the first, however, the percentage of complications after such treatment is also close to 99%, and you also need to run.
- Method of lethal condensation of cold gutta-percha - the meaning of this method is to compact the pins of cold gutta-percha as tightly as possible along the entire length of each of the root canals. We will discuss this method in more detail below. The method has an affordable cost and high reliability.
- Vertical condensation of hot gutta-percha is the most effective method of filling canals, which is carried out using gutta-percha heated to a fluid state.
The latter then gradually cools and hardens. Due to the fact that at the beginning it is in a fluid state, gutta-percha flows even into the lateral microchannels, which cannot be sealed by any other method (even the lateral condensation method). There are many techniques for using this method and materials for it. However, the best system for filling canals with hot gutta-percha called Termafil. If you are willing to pay for quality and reliability, then this is your method. But be prepared for the fact that the cost of filling canals with Termafil will be high.
Video: filling canals with cold and hot gutta-percha
Upper second premolar
Upper second premolar. (I channel configuration type).
This tooth tends to be single-rooted. Type I of the canal configuration prevails, but in 25% types II and III are present, and in 25% there may be types IV - VII with two apical openings.
Thus, the basic type of this tooth can be considered as single-rooted with a single canal. Rarely, there may be two roots, and then the tooth resembles a first premolar with the bottom of the cavity located significantly below the neck of the tooth. The average length is slightly longer than the length of the first premolar and averages 21.5 mm.
The pulp chamber is expanded in the bucco-palatal direction and has two pronounced horns. Compared to the first premolar, the bottom of the chamber is located closer to the apex.
The root canal is wider in the bucco-palatal direction and narrower in the mediodistal direction. It tapers towards the apex, rarely round in cross-section, with the exception of two or three mm at the apex. Often the root of this single-rooted tooth is divided into two sections by a groove in the middle third of the root. These sections are connected almost without variations and form a common canal with a relatively large apical opening. The canal is usually straight, but the apex may have a curvature distally and, less commonly, buccally.
With age, the displacement of the roof of the pulp chamber is the same as in the first premolar.
Method of lethal condensation of cold gutta-percha -
In Russia, 95% of all root canals are filled using this method.
The method of lethal condensation consists in the doctor performing a number of stages, the success of which largely depends solely on the high-quality implementation of the previous stages. We are talking about the correct measurement of the length of the root canal, as well as the quality of the instrumentation performed. Lateral condensation of gutta-percha (scheme) –
- Selection of the main gutta-percha pin - the pin is selected depending on how much the root canal was expanded during mechanical treatment)
- Filling the root canal with sealer – sealer is a special paste that is used to fill the voids between gutta-percha pins. After introducing the sealer, the main pin is inserted into the canal (Fig. 14a)
- Compaction of a gutta-percha pin with a spreader - the compaction process consists of making reciprocating movements with the spreader instrument, with its help the gutta-percha is pushed towards the canal wall and space is freed up for the insertion of new gutta-percha pins. The spreader itself is shown in Fig. 14(b), and the compaction process in Fig. 14(c).
- Insertion of smaller pins and their compaction (Fig. 14 d, e, f) - up to 8-12 gutta-percha pins can be “compacted” in just one root canal. As a result, if we look at an enlarged section of the tooth root, we should see a picture like this - Fig. 17.
- X-ray control of filling - if everything is OK - we proceed to the next stage... But if we see that the canal is not filled to the top, or the pins extend beyond the root into the surrounding tissues - it is necessary to remove all the pins and start filling the canals from the beginning.
- Removing excess gutta-percha and sealer - after the canals are tightly obturated with gutta-percha and sealer, the tips of the gutta-percha pins protruding from the mouths of the root canals are cut off with a hot tool (Fig. 14 g, h). You can see what the mouths of the root canals look like before filling and after they have been cut, excess gutta-percha protruding above the mouths of the canals in Fig. 15 and 16, respectively.
- Temporary filling – After this, the tooth cavity is closed with a temporary filling. It is not allowed to fill the crown of a tooth in the same visit with filling the canals. Restoration of the tooth crown should be carried out at the next visit.
Lower canine
Lower canine. (I channel configuration type). (By Harty).
This tooth resembles the upper canine, although its size is smaller. Very rarely it has two roots. Its average length is 22.5 mm. Type I canal is the most prevalent, but the main deviation in canines is the variant with two canals (frequency about 14%). In less than 6% of cases, a type IV canal configuration with two separate apical foramina is found.
Access to lower incisors and canines
Essentially, the approach is identical to that in the upper teeth. However, with a pronounced curvature towards the lingual side of the crowns of the incisors and due to very thin (especially in older people) canals, it is sometimes necessary to involve the cutting edge and, sometimes, the labial surface of the tooth into access to avoid bending of the instrument.
The outlines of the access in the lower canine are shown in Fig.
Access contours in the lower incisors.
Access contours in the lower canine.
Lower premolars
These teeth usually have a single root, but sometimes the first premolar may have a bifurcated root in the apical half.
Type I channel predominates. Where there are two canals (usually in the first premolar), there may be type IV/V configurations. Types II/III occur in less than 5% of cases. The highest incidence of two canals is reported to be 10.8% in the second premolar (Zillich and Dowson, 1973).
One report found that two canals in the first premolar were three times more common in African-Americans than in whites (Trope et al., 1986). This option is more common among southern Chinese. In less than 2%, three canals may be present in the first premolar.
The pulp chamber of the lower premolars is wider in the buccolingual direction than in the mesiodistal direction, and has two horns, the buccal one being better developed. The lingual horn is small in the first premolar and larger in the second premolar.
Lower first premolar. (II channel configuration type). (By Harty).
The canals of the lower premolars are similar to the canines of the canine, although they are smaller, but they are also wider in the bucco-lingual direction until the middle third of the root, when they narrow and acquire either a rounded shape or bifurcate.
Lower second premolar. (I channel configuration type). (By Harty).
Lower second molar
In Caucasians, the second molar resembles a small version of the first, with an average length of 20 mm. There are two canals in the medial root, and only one in the distal root. The medial canals tend to merge in the apical third and form a single apical foramen.
Lower second molar. (By Harty).
Studies conducted in 1988 showed a high tendency for root fusion in the Chinese (33-52% of cases). In a longitudinal section, such teeth resemble a horseshoe. Where there is incomplete root separation, incomplete canal separation may occur, which is accompanied by a dense network of anastomoses between the canals and can lead to unpredictable localization of the orifices. One of the locations was called the middle buccal orifice with the middle buccal canal. In Caucasians, this anomaly is recorded in 8% of cases, which is significantly less than in the Chinese.
Lower third molar
This tooth is often underdeveloped with numerous and poorly developed cusps. Usually there can be as many canals as there are cusps. The root canals are relatively larger than those of other molars, possibly due to the late development of this tooth.
Despite these disadvantages, it is usually less difficult to fill the roots of a lower than an upper wisdom tooth because access is usually easier due to the mesial inclination of the tooth and because they more often follow normal anatomy, resembling a second molar, and are less likely to be deviated from the norm.
How to save teeth?
- To keep your teeth healthy, you need to properly organize your diet, including foods rich in proteins, amino acids, vitamins, calcium and phosphorus.
- Carry out oral and dental hygiene regularly and thoroughly. Change your toothbrush every three months, choosing one with bristles that are more suitable for your teeth. Choose a good toothpaste and teeth rinse. You should definitely brush your teeth immediately after sleep and before bed. After each meal, you should rinse your mouth or chew gum.
- If your teeth are healthy, you should visit a dentist once a year, who will conduct a visual examination of your teeth, remove plaque or tartar, and give recommendations on how to care for your teeth.
Be that as it may, if there is pain or discomfort in the teeth, then you need to seek help from a dentist. This will help to eliminate the problem in time and get rid of the causes of pain.