Canal unsealing is a dental procedure that is aimed at removing a previously installed filling. Another name for it is “disobturation”. The process requires expansion of the canals in the direction from the crown to the apex of the root for the purpose of high-quality cleaning of dental cavities. The procedure is resorted to after endodontic treatment carried out with violations of technology. It must be carried out on time, since infectious agents that have penetrated the dental tissues will provoke the development of inflammatory processes, which, in turn, can cause the loss of the entire tooth.
The therapeutic department of dentistry CELT invites you to undergo root canal retreatment in Moscow. Our clinic is multidisciplinary and has been offering paid medical services for more than two decades. Our dental therapists have a modern diagnostic and treatment base in their arsenal, thanks to which they are able to accurately and promptly make diagnoses and carry out treatment in accordance with international standards. You can find out the approximate price for unsealing canals by going to the “Services and Prices” tab. We regularly update the price list, but in order to avoid misunderstandings, we recommend that you check the exact numbers with our operators or at a doctor’s appointment.
Consultation with a dentist-therapist - 1,000 rubles.
Unsealing a previously obstructed canal (1 canal) - RUB 3,000.
Unsealing the canal under the stump tab - 1,700 rubles.
At CELT you can get advice from a dental specialist.
- The cost of a consultation with a dentist-therapist is 1,000
Make an appointment
Indications and contraindications for root canal filling
Indications
- Painful symptoms, inflammatory processes and swelling of the gum tissue in a patient who some time ago underwent endodontic treatment;
- Insufficient quality of the filling is its depressurization or poor fit at the edges, which makes it difficult to remove food debris and provokes the development of a carious process;
- Inflammatory or infectious processes of the dental canals under the filling;
- The need for retreatment of root canals for pulpitis, periodontitis, cystic formation, granuloma;
- The need to install an intracanal pin;
- Violations of the previously performed root canal obturation technology.
Contraindications
- Serious damage to the periodontal tissues surrounding the unit, which is not an obstacle to saving the tooth;
- The unit is unsuitable for restoration;
- Impossibility of intervention on its closed part;
- Neoplasm of malignant etiology in the area of the affected unit;
- A purulent-necrotic process that affects bone tissue;
- General serious condition of the patient.
Situations requiring disobturation
The dentist will learn about the need for repeated endodontic treatment by a variety of symptoms. One of these symptoms is the presence of pain in the treated tooth. We are not talking about temporary pain, which often accompanies the patient in the first 2-3 days after treatment, but about permanent pain.
The need for repeated intervention is also indicated by the appearance of infectious and inflammatory processes in the tooth. This is established during a delayed X-ray examination or when the patient complains. Similar diseases include caries, periodontitis, inflammation under the crown.
Swelling of the gum tissue at the location of the tooth is also considered a symptom. Poor condition of the filling that covers the root canals and its loosening. This happens when the edge fit of the material is unstable.
The same procedure may be required if it is necessary to install a channel pin. Depressurization of the filling material and darkening of the tooth lead to repeated intervention. Poor quality work by the dentist when applying the filling for the first time, as well as incomplete filling of the canals with it, is also considered an indication.
Features and stages of unfilling root canals using medication
Chemical deobturation is carried out using one of two methods:
- Moderate complexity - performed in one visit and indicated if you need to remove hardening pastes. The latter dissolve well with organic solvents and are easily removed using endodontic instruments. In this case, canal retreatment under a microscope is carried out in one visit to the dentist;
- High complexity - indicated if the canals were filled with cement or resorcinol-formalin paste, rarely required when treating patients with old fillings. A dissolving gel is instilled into the canal, and after the filling has softened, a special tool is inserted into it, which allows it to be removed by turning it clockwise and counterclockwise. The dentist must work very carefully so as not to damage the integrity of the canal walls or break the instrument. This type of filling requires two visits to the doctor.
Stages of chemical unsealing:
- Removing a surface filling with a dental bur;
- Applying solvent to old material;
- Careful removal of the filling material after it has softened;
- Removal of tissue affected by caries, treatment of other diseases;
- Re-filling of canals.
Concept of procedure
The procedure for removing old fillings from dental root canals is called disobturation. The filling is completely removed, after which all dental cavities are cleansed of its remains. The future fate of the diseased tooth depends on the quality of such actions.
During the procedure, special instruments are used to clean from the crown of the tooth to the apical part. In this case, expansion is carried out first with smaller devices, and then with larger ones. Only in this option will cleaning be complete and effective.
Reviews of doctors providing the service - root canal unfilling
I would like to express my gratitude to the dentist Elena Nikolaevna Kiseleva and her assistant Svetlana - they are real specialists and at the same time sensitive, not burnt out by years of practice.
Thanks to them, I have been coming back here for many years. Thanks to the management for such doctors! Read full review Svetlana Nikolaevna
13.08.2021
Words cannot express my gratitude to Elena Nikolaevna Kiseleva. This is the best doctor in the world. I got an appointment after many years of being ignored by the dentist’s office and with a bitter experience of treatment in another paid clinic, the mistakes of which had to be corrected in the first visits. Thank you for this... Read full review
Roman Stanislavovich Sh
25.07.2020
Possible complications
Unfilling the canal is associated with the risk of tooth perforation. This is the formation of an artificial hole between the root or crown of the tooth and the periodontal ligament. Occurs due to medical error at the stage of creating endodontic access without root canal topography.
Another possible complication is the presence of broken parts of dental instruments. In this case, it is necessary to remove the foreign body, since the metal corrodes and irritates the walls of the dental canal, which can lead to the formation of cracks in the tooth root or its premature loss.
Complications are also possible with late opening of the tooth cavity into the root canal. Advanced caries, periodontitis, and low-grade inflammation increase the risk of tooth loosening and loss. Therefore, it is important to unseal the canal as soon as possible if there are indications.
Why is the procedure so effective?
With the right approach, the procedure allows you to save the tooth due to:
- removal of tissue affected by caries;
- no need for anesthesia;
- eliminating the symptoms of diseases that developed under the filling
The use of a microscope in the process significantly improves its quality, since it allows you to correctly assess the features of the anatomical structure and the condition of the root canals. It is worth noting that the cost of canal retreatment with their use is higher, however, the effectiveness of the procedure increases significantly.
Indications
Opening the tooth cavity into the root canal is necessary for re-treatment of the tooth.
The main reasons for unfilling the canal:
- resorption of filling material;
- poor quality filling;
- violation of the treatment of the tooth cavity;
- high-shrinkage fillings that create space over time;
- the occurrence of deep caries, periodontal disease;
- incomplete depulpation;
- an unevenly processed filling that constantly irritates the periodontal tissue;
- penetration of infection into the dental ligament;
- root perforation.
What matters is the quality of hygienic care for the oral cavity, the susceptibility of tooth tissue to caries, the presence of foci of chronic infections, the general condition of the body, as well as insufficient knowledge and qualifications of the dentist.
Unsealing of the tooth canal will be required before installing the core inlay at the stage of taking the impression. Consultation with a dentist-therapist is necessary if the color of the filling changes, its marginal fit is poor, the formation of cracks and chips, inflammation of the gums, or carious lesions of the tooth. Painful sensations also force patients to see a dentist.
Removing the seal under the anchor pin
Obturation of the tooth root canal is done in parallel using anchor pins. If the filling in the lower part of the root is placed correctly and hermetically, then it is left to install the pin structure. This procedure is carried out over two trips to the dental office.
On the first day, the doctor treats the dental canal mechanically, softens the filling with medications and cleans the passage with an endo-instrument. The doctor then soaks a cotton swab in the medicine and inserts it into the canal. The patient takes the medicine for a couple of days and then makes another visit to the doctor, during which the cotton swab is removed and the canal is refilled.
Modern technologies in the field of tooth refilling
Dental treatment under a microscope is one of the newest services that has appeared in dentistry. High-tech equipment allows specialists to fill the dental canal with better quality, more accuracy and efficiency. Thanks to the use of such a device, the likelihood of causing harm to healthy tissue is close to zero. In addition, the treatment is carried out very delicately. Microscope glasses allow you to view the tooth at multiple zooms. This will allow you to see all the affected areas that may simply not be visible during normal examination.
A microscope allows dentists to perform root canal treatment faster and safer for the patient.
Modern techniques
Unsealing root canals provides for the possibility of using two techniques:
- Chemical desobturation is a procedure during which a layer of paste or a special solution is applied to the filling material, softening its structure;
- Mechanical filling removal involves the use of dental equipment to remove material from the crown and root.
A prerequisite is antiseptic prophylaxis of the oral cavity, as well as, if necessary, treatment of the tooth with a drill or root reamer.
Features of the procedure for re-treatment of a dental canal
Refilling the canal of a previously treated tooth is a special case in the practice of dentists. Before doing this, it is necessary to remove the old filling, clearing the entire dental canal of the filling material. During such work, the flexible rod may break. This will somewhat complicate the dental treatment process.
Typically, this problem occurs with a very dense filling that is closely adhered to the walls of the canal of the tooth being treated.
Difficulty also arises if it is necessary to refill curved dental canals. When cleaning such channels, you can damage their walls or even break the instrument. Such situations require increased attention from the specialist to ensure high-quality completion of the canal filling. Specialists are required to inform the patient about possible difficulties during treatment before the procedure.
Where to unseal canals in Moscow
Beskudnikovo Dentistry employs doctors who specialize in the treatment of root canals, including those of complex anatomical structure. Our dentists use modern equipment, effective and safe medications, and high-tech instruments to open the tooth cavity and re-treat it.
If there are anatomical features of the canal, all manipulations are carried out under a microscope. The device provides an enlarged image several times, which eliminates medical errors, guarantees high quality treatment, and minimizes the risk of injury to tooth tissue. The cost of filling a tooth canal with a microscope is higher than conventional treatment, so the exact cost is discussed with the doctor during a free initial consultation.
Preparation of root canals. 5th generation of instruments
ROOT CANAL PREPARATION
5 GENERATION OF INSTRUMENTS Dr. Clifford J. Ruddle (USA)
Doctor of Dentistry (DDS), Fellow of the International College of Dentists (FICD), Fellow of the American College of Dentists (FACD)
With the participation of:
Dr. Pierre Machtou (France Doctor of Dentistry (DDS), Master of Science (MS), PhD, Fellow of the International College of Dentists (FICD) Dr. John West (USA)
Doctor of Dentistry (DDS), Master of Science (MSD), Director of the Center for Endodontics
Dr. Clifford J. Ruddle is the founder and director of Advanced Endodontics, an international educational resource, in Santa Barabara, California.
He is an assistant professor of endodontics at Loma Linda University and the University of California, Los Angeles, a clinical associate professor at the University of California, San Francisco, and an associate professor of endodontics at Pacific University School of Dentistry. As an inventor, Dr. Ruddle has developed and improved several tools and devices that are widely used throughout the world. He is well known as an excellent teacher of endodontics, with lectures, clinical articles, tutorials, videos and DVDs in his arsenal. He also has a private practice in Santa Barbara, California. In the early days of modern endodontics, there were many concepts, strategies, and techniques for root canal preparation. Over the past decades, dozens of tools for passing and shaping canals have appeared.
The breakthrough in clinical endodontics occurred with the transition from the use of a long series of stainless steel instruments and multiple Gates Glidden reamers to the use of nickel titanium instruments for canal preparation. Regardless of the techniques used, the goals of mechanical root canal treatment were brilliantly defined almost 40 years ago by Dr. Herbert Schilder1.
With the correct treatment algorithm, mechanical treatment of root canals should correspond to the biological goals of canal preparation, three-dimensional disinfection and obturation (Figure 1).
The purpose of this article is to demonstrate and compare new generations of endodontic nickel titanium instruments designed to improve root canal preparation. It is important that this article will define a new tool system that combines proven design features of the past with the latest innovations of the present, and the operating technique will also be described.
Rice.
1a. Micro computed tomography of the upper central incisor demonstrates a root canal system with multiple exits serving as support for the root apex. Rice. 1b. The radiograph before treatment shows unsatisfactory endodontic intervention on the anterior tooth and denture. The tooth has a fistulous tract.
Rice. 1c. This image after the retreatment procedure shows the importance of shaping the root canals, which contributes to better three-dimensional cleaning and obturation.
Rice. 1d. An X-ray 25 years after treatment demonstrates healing of the bone tissue.
PREPARATION OF ROOT CANALS WITH NI-TI INSTRUMENTS
In 1988, Walia introduced Niti-Nol, a nickel-titanium alloy for root canal preparation that is 2-3 times more flexible than stainless steel alloy for the same instrument sizes.
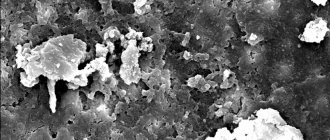
A revolutionary result of the use of instruments made of nickel-titanium alloy was the ability to machine curved canals using continuous rotation. By the mid-1990s, the first commercially available nickel-titanium rotary tools appeared on the market. Below is a mechanical classification of each generation of instruments. Rather than describe the myriad of tool cross-sections that exist, we will differentiate between tools with passive and active cutting capabilities. Rice. 2. These scanning electron microscope images show the cross section and lateral view of a passive cutting tool with radial edges. Rice.
3. These scanning electron microscope images show the cross section and lateral view of the active tool with sharp cutting edges. FIRST GENERATION
To appreciate the evolution of nickel-titanium tools, it is useful to know that the first generation of nickel-titanium tools had passive radial cutting edges and fixed tapers of 4% and 6% along the entire length of the active blades (Figure 2). This generation required a variety of instruments to achieve dissection goals. In the mid to late 1990s, GT instruments (Dentsply) were introduced which had a fixed taper on each individual instrument of 6%, 8%, 10%, and 12%. The single most important design feature of the first generation of nickel-titanium rotary instruments was the passive radial edges, which allowed the instrument to remain centered in the curvature of the root canal during operation.
SECOND GENERATION
The second generation of nickel-titanium rotary tools came onto the market in 2001. The main difference with this generation of instruments is that they have active cutting edges and only a few instruments are required to complete a complete root canal preparation (Figure 3). To avoid the locking cone and resulting screw-in effect associated with passive and active tapered NiTi instruments, EndoSequence (Brassler) and BioRaCe (FKG) offer instrument lines with alternating contact points.
Although this characteristic is intended to reduce the effect of the locking cone, these lines of tools have a fixed taper in the area of the active cutting part. A clinical breakthrough occurred when the ProTaper (Dentsply), which has multiple increasing and decreasing tapers throughout a single instrument, came to market. This revolutionary progressive taper shape limits the cutting action of each instrument to a specific section of the canal, allowing the use of a shorter sequence of instruments to safely reproduce the Schilder canal shape (Figure 4).
Rice. 4. ProTaper root canal shaping instruments work primarily in the coronal and middle thirds of the canal, while finishing instruments work primarily in the apical third of the canal.
During this period, manufacturers began to actively seek methods to improve tool strength. Some manufacturers have used electropolishing on their tools to remove surface irregularities created by the traditional tool grinding process. However, through clinical observations and scientific research, it was found that electropolishing dulls cutting edges. As such, the observed benefits of electropolishing were offset by the need to apply unwanted pressure inside the root canal to advance the instrument to its full working length. Excessive internal pressure, especially when using fixed taper tools, results in a locking cone effect, a screw-in effect, and excessive torque on the rotating tool during operation. To compensate for the shortcomings or ineffective operation of the tool as a result of electropolishing, other cross-sections of the tools were proposed and the rotation speeds, despite all the dangers, were increased.
THIRD GENERATION
Improvements in the metallurgy of nickel-titanium alloys have become the hallmark of the third generation of instruments for mechanical treatment of root canals. In 2007, manufacturers focused on heating and cooling processes for the alloys to reduce cyclic fatigue and improve safety when working with nickel-titanium instruments in more curved root canals. The desired point of phase transition between martensite and austenite can be identified with the search for a clinically more optimal metal than nickel-titanium. This third generation of nickel-titanium instruments is characterized by a significant reduction in cyclic fatigue and, accordingly, instrument fracture. Examples of heat treated instruments include Twisted File (SybronEndo), Hyflex (Coltene Whaledent) and GT, Vortex, and WaveOne (Dentsply).
FOURTH GENERATION
Another progressive movement in canal preparation is reciprocation, which can be defined as any repeated back-and-forth or up-and-down movement. This technology was first introduced in the late 1950s by the French dentist Blanc. Today, M4 (SybronEndo), Endo Express (Essential Dental Systems), and Endo-Eze (Ultradent) are examples of systems where the clockwise rotation angle of the instrument is equal to the counterclockwise rotation angle of the instrument. Compared to full rotation systems, a reciprocal instrument that rotates at equal angles clockwise and counterclockwise requires more pressure into the root canal to move forward, does not cut as efficiently as a rotary instrument of the same size, and is more limited in removing sawdust and debris from the root canal. channel.
Based on these early experiences, reciprocation technology has steadily developed, leading to the creation of the 4th generation of root canal preparation instruments. This generation of instruments and reciprocation technology are embodied in the much-anticipated one instrument. ReDent-Nova (Henry Schein) introduced the Self-Adaptive Instrument (SAF). This instrument has the shape of a compressible hollow tube; it is assumed that the instrument exerts uniform pressure on the dentinal walls, regardless of the cross-section of the canal. The SAF instrument is mechanically rotated by a handpiece that performs both short 0.4 mm vertical movements and vibration movements with continuous irrigation11. Another promising single tool technique is called One Shape (Micro Mega), which will be mentioned below in the chapter on 5th generation tools.
By far the most popular single instrument concept is the WaveOne (Dentsply) and Reciproc (VDW) system. WaveOne combines the best design features of 2nd and 3rd generation tools with a reciprocal motor that rotates any tool back and forth at unequal angles. The angle of movement counterclockwise is 5 times greater than the angle of movement clockwise, and it is less than the elastic limit of the tool. After 3 cycles of counterclockwise and clockwise rotations, the tool will make a full circle or 360° rotation (Figure 5). This new reciprocal movement allows the instrument to easily advance, effectively process and remove sawdust from the root canal.
FIFTH GENERATION
The fifth generation of canal preparation instruments differs in that the center of gravity and/or the center of rotation is shifted (Figure 6). When tools with a similar shape rotate, a mechanical wave of motion arises, which moves along the entire length of the tool. Like progressive
Rice. 5. The WaveOne reciprocal instrument uses unequal clockwise and counterclockwise rotation angles to improve efficiency, advance into the root canal and extract sawdust from the root canal.
Rice. 6. Cross section of the ProTaper Next instrument. Note the off-center mass of the tool, which reduces screwing into the channel, provides more space for sawdust and improves flexibility.
Taper of any ProTaper instrument, the shifted center of gravity further minimizes friction between the instrument and the dentin. Also, this design improves the removal of sawdust from the canal and improves the flexibility of the active part of the Protaper Next tool. The advantages of tools with a shifted center of gravity will be described later in this article.
The trade names for instruments based on this technology are Revo-S, One Shape (Micro Mega) and ProTaper Next (Dentsply Maillefer). Today's safest, most effective, and simplest tool systems utilize the time-tested features of past generations of tools combined with the latest technological advances. Below is a brief technical description of the ProTaper Next system.
PROTAPER NEXT
The new ProTaper Next (PTN) system (Dentsply Maillefer) features 5 instruments of varying lengths for root canal preparation, labeled X1, X2, X3, X4, and X5 (Figure 7). From 1 to 5 they are color coded yellow, red, blue, double black and double yellow stripes on the handle, corresponding to sizes 17/04, 25/06, 30/07, 40/06, and 50/06 , respectively. The taper listed is NOT fixed across the entire working portion of the ProTaper Next tool. Imagine that the ProTaper Next X1 and X2 instruments have both an increasing and decreasing taper throughout the same instrument, while the ProTaper Next X3, X4 and X5 instruments have a fixed taper for the first 3 mm of length, and then a decreasing taper for the entire remaining active part.
ProTaper Next tools are a combination of 3 significant design features such as increasing taper on the same tool, M-wire technology and an off-center section. As an example
Rice. 7. The illustration shows a sequence of 5 ProTaper Next tools. Most root canals on posterior teeth can be created with 2–3 instruments.
Take the ProTaper Next X1 tool, it has a centered mass and axis of rotation over the first 3 mm of length, whereas from 4-16 mm the X1 tool has a displaced cross-section. From 1 to 11 mm, the X1 instrument increases its taper, starting at 4%, while from 12 to 16 mm there is a decreasing taper to improve instrument flexibility and preserve root dentin during root canal preparation procedures.
ProTaper Next tools are used at 300 rpm. and torque from 2.0-5.2 N cm. However, the authors prefer a torque of 5.2 Ncm because this level of torque has been found to be safe as long as clinicians carefully create a carpet path and use gentle sweeping movements during progressive root canal preparation. 14 In the ProTaper Next technique, all instruments are used exactly the same and the sequence of use always follows the ISO color code and is always the same regardless of length, diameter, or curvature.
Rice. 8a. The radiograph shows a tooth that is supporting a bridge in the lateral region and is in need of endodontic treatment. Pay attention to the orientation of the denture relative to the roots.
Rice. 8b. The work in progress picture shows the removal of the crown, isolation and No. 10 instruments inserted into the root canals, which have different curvature radii.
Rice. 8c. This photograph shows a mechanical wave of motion moving along the active portion of the ProTaper Next X1 instrument.
PROTAPER NEXT PREPARATION TECHNIQUE
The ProTaper Next preparation technique is extremely safe, effective and simple, provided the access cavity is good and a carpet is created. As with any root canal preparation procedure, great care must be taken to create straight, linear access to each orifice. This involves widening, smoothing and finishing the internal axial walls. For estial access, the ProTaper system offers an additional instrument called the SX. The SX instrument is used in an outward sweeping motion to preliminarily widen the orifice, remove dentin triangles, move the coronal portion of the canal away from the outer curvature of the root, or create a more pronounced shape. Perhaps the greatest challenge in endodontic treatment is finding, following and predictably maintaining the shape of the root canal to the apex. Traversing and maintaining the shape of the canal using fine hand instruments requires mechanical strategy, an experienced sense of work, patience and desire. A small hand-held tool is initially used to explore, widen and smooth the inner walls of the canal. Once the entire length of the root canal is passable with a hand instrument, a continuous rotation instrument can be used to create a carpet and widen the original canal opening in preparation for shaping. To be clear, a channel is only prepared when it is empty and has a proven smooth and repeatable carpet.
With an estimated working length and in the presence of a viscous chelating agent, insert a #10 K-file instrument into the root canal and see how easily the instrument moves toward the apex of the root canal.
In shorter, wide and straight canals, the No. 10 instrument can be easily inserted to the full working length. Once it has been confirmed that it moves freely to its full working length, the carpet can be further widened either with a size 15 hand tool or with specially designed tools such as PathFile (Dentsply). The created carpet path provides sufficient space to begin machining with the ProTaper Next X1 tool.
In other cases, teeth requiring endodontic treatment may have longer, narrower, and more curved root canals (Figure 8a). In such situations, the No. 10 instrument often does not penetrate the entire length of the root canal. It is generally not necessary to use #06 and/or #08 hand instruments in an attempt to immediately reach the apical foramen. Simply and gently work the #10 hand instrument within any area of the root canal until the instrument is completely free. ProTaper Next instruments can be used to create any part of the root canal with a smooth and reproducible carpet. Although there is a glide path and a sequence of instrumentation, the ultimate goal is to complete the entire working length of the root canal, establish the working length, and check for apical patency (Figure 8b). Safe work with the canal can begin after checking the created carpet, when tool No. 10 does not stick at the working length and can slide and move again in the area of the lower third of the root canal.
When the canal is prepared, the access cavity is generously filled with a 6% NaOCl solution. You can begin canal preparation with the ProTaper Next X1. It should be emphasized that when working with ProTaper Next instruments, pumping or pecking movements directed inward are never used. In contrast, ProTaper Next tools are used in an outward sweeping motion. It is important that this method of use will allow any ProTaper Next tool to move passively inwards, following a carpet path and penetrating the entire working length. Instrument X1 is inserted into the access cavity into the previously expanded orifice and prepared canal. Before meeting resistance, consciously begin sweeping outwards (Figure 8c). Sweeping creates lateral space and allows this tool to penetrate a few millimeters inside. Sweeping movements serve to improve contact between the instrument and dentin, especially in canals with a non-standard cross-section.
Continue working with the ProTaper Next X1 along the main part of the root canal. As you immerse the tool every next few millimeters, remove it and examine it while simultaneously cleaning the blades. Before re-inserting instrument X1 into the root canal, it is strategically important to irrigate and wash out large sawdust, as well as reintroduce instrument No. 10 in order to destroy residual sawdust and decay products and put them into solution, then re-irrigate to update the solution. In one or more passes you should reach the working length of the X1 tool. For thorough mechanical preparation purposes, irrigate, recapitulate, and re-irrigate after removing any rotating instrument.
Rice. 8d. This photograph shows the ProTaper Next X2 inserted to its full working length in the mesiobuccal canal.
Rice. 8e. This photograph shows the ProTaper Next X3 inserted to its full working length in the distal canal.
Rice. 8f. This radiograph demonstrates the temporary fixation of the bridge, the smoothly created shape of the root canals, and the importance of root canal treatment.
Take the ProTaper Next X2 and let it sink into the root canal. Before resistance is encountered, apply a lateral sweeping motion away from the dentinal walls, which in turn will move the X2 instrument into the root canal passively and progressively. The X2 tool will easily follow the path created by the X1 tool, making further expansion and gradually moving along the entire length. If the tool gets stuck and stops moving, remove it, clean it and check the edges. Re-irrigate, recapitulate, and re-irrigate to meet channeling goals. Continue working with tool X2 until working length is reached; note that one or more approaches may be required, depending on the length, width and curvature of the canal (Figure 8d).
Once the ProTaper Next X2 has reached working length, it is removed. The created form can be considered final only if the grooves in the apical part of the instrument are visually filled with dentin.
Alternatively, the apex size can be checked with a 25/02 hand instrument. If the #25 hand instrument sticks at the working length, the preparation is complete. If the 25/02 hand tool moves freely at working length, this simply means that the apical foramen is wider than 0.25 mm. In this case, the apex can be calibrated using a size 30/02 hand tool. If the #30 size hand tool sticks at the working length, the mold is created. However, if a #30 size hand tool does not reach the apex, move on to the ProTaper Next X3 tool, following the same operating procedure as with the ProTaper Next X1 and ProTaper Next X2.
Most root canals will be in optimal shape after using ProTaper Next X2 or X3 (Figure 8e). The ProTaper Next X4 and X5 instruments are primarily used for the preparation and finishing of larger diameter root canals. If the apical foramen is determined to be larger than the ProTaper Next 50/06 X5 size, consider other methods for preparing similar wide, straighter canals. It is important to recognize that carefully prepared canals promote shaping, three-dimensional cleaning and obturation (Figure 8f).
DISCUSSION
From a clinical point of view, the Protaper Next continuous rotation system combines the most proven and successful design features of past instruments with the latest advances in science. This brief discussion will describe how design affects instrument performance.
The most successful design feature of the previous generation of instruments was the mechanical concept of using progressive taper on the same instrument. The patent protecting the ProTaper Universal system allows the use of both increasing and decreasing taper percentages on the same tool. This structural feature minimizes contact between the instrument and dentin, which reduces the risk of a locking cone and screw-in effect, increasing work efficiency. Compared to a fixed taper instrument of the same size, decreasing the percentage of instrument taper improves flexibility, limits preparation of the root canal body, and preserves dentin in the coronal 2/3 of the root canal. Taking advantage of the mechanical design, Protaper Next also uses progressive taper on the same tool. This design feature has contributed significantly to the ProTaper system becoming the #1 selling system in the world, the #1 tool of choice for endodontists, and the #1 system of choice for undergraduate dental school education at international schools.
Another design feature that benefits certain brands of rotary tools is metallurgy. Although nickel-titanium tools are 2 to 3 times more flexible than stainless steel tools of the same size, additional modifications to the manufacturing process in the form of heat treatment can provide certain benefits. The company's specialists paid attention to the heating and cooling of a traditional nickel-titanium alloy either before or after milling. Heat treatment creates a more optimal phase transition point between martensite and austenite. It must also be remembered that the best phase transition point depends on the cross section of the tool. Research has shown that M-wire, a metallurgically enhanced version of nickel-titanium alloy, reduces cyclic fatigue by 400% compared to tools of the same diameter, cross-section and taper. This third benefit of this generation of instruments is strategic for the overall clinical safety and performance of the Protaper Next rotary instrument system.
The third design feature of Protaper Next tools is the off-center cross section. If the main part of the continuous rotation tool is off-center, we can talk about 3 advantages of this:
1) Off-center cross-section contributes to the formation of a moving mechanical wave of motion along the entire active part of the tool. This rocking motion promotes minimal contact
Rice. 9. ProTaper Next features an off-center cross-section and progressive taper. These characteristics minimize tool screwing, increase the volume of sawdust extracted and improve flexibility. For comparison, the figure below shows a tool with a fixed taper, centered mass and axis of rotation.
Rice. 10. Like a sine wave, the ProTaper Next rotary tool creates a mechanical wave of motion or rocking effect along the active part of the tool.
Instrument and dentin compared to instrument motion with a fixed taper and mass-centered rotation (Figure 9). Reduced contact limits unwanted locking taper, screw-in effect and torque on any tool.
2) An instrument with an offset section frees up more space for dentinal filings from the root canal compared to an instrument with a centered mass and axis of rotation (Figure 9). Many tools break as a result of excessive accumulation of sawdust and debris between the cutting blades throughout the active part of the tool. It is important that an off-center instrument reduces the likelihood of lateral compaction of sawdust and blocking of the root canal anatomy (Figure 6).
3) A forming tool with an off-center rotation mass will create a mechanical wave of motion similar to vibrations recorded along a sinusoid (Figure 10). As a consequence of this design, any Protaper Next tool can create a greater range of motion compared to a similar tool with a symmetrical mass and axis of rotation (Figure 6). The clinical advantage of this is that the smaller, more flexible Protaper Next instrument can prepare a similar space to a larger, more rigid instrument with a centered mass and axis of rotation (Figure 9).
CONCLUSION
Each new generation of shaping tools offers something new, is described differently, and is intended to be an improvement over the previous one. Protaper Next is a 5th generation system that combines the proven performance characteristics of the past with the latest technological advances. This system should simplify the procedure of canal formation with rotary instruments, reducing the number of instruments and eliminating the so-called hybrid techniques. Clinically, the canal shape created by Protaper Next fulfills the 3 sacred dogmas: safety, effectiveness and simplicity. From a scientific perspective, evidence-based studies are needed to confirm the potential benefits of the system.
BIBLIOGRAPHY:
1. Schilder H: Cleaning and shaping the root canal, Dent Clin North Am 18:2, pp. 269-296, April 1974.
2. Walia HM, Brantley WA, Gerstein H: An initial investigation of the bending and torsional properties of Nitinol root canal files, J Endod 14:7, pp. 346-351, 1988.
3. Thompson SA: An overview of nickel-titanium alloys used in dentistry, Int Endod J 33:4, pp. 297-310, 2000.
4. Bryant ST, Dummer PM, Pitoni C, Bourba M, Moghal S: Shaping ability of .04 and .06 taper ProFile rotary nickel-titanium instruments in simulated root canals, Int Endod J 32:3, pp. 155-164, 1999.
5. Kramkowski TR, Bahcall J: An in vitro comparison of torsional stress and cyclic fatigue resistance of ProFile GT and ProFile GT Series X rotary nickel-titanium files, J Endod 35:3, pp. 404-407, 2009.
6. Machtou, P, Ruddle CJ: Advancements in the design of endodontic instruments for root canal preparation, Alpha Omegan 97:4, pp. 8-15, 2004.
7. Schfer E, Vlassis M: Comparative investigation of two rotary nickel-titanium instruments: ProTaper versus RaCe. Part 2. Cleaning effectiveness and shaping ability in severely curved root canals of extracted teeth, Int Endod J 37:4, pp. 239-248, 2004.
8. Ruddle CJ: The ProTaper endodontic system: geometries, features, and guidelines for use, Dent Today 20:10, pp. 60-67, 2001.
9. Boessler C, Paque F, Peters OA: The effect of electropolishing on torque and force during simulated root canal preparation with ProTaper shaping files, J Endod 35:1, pp. 102-106, 2009.
10. Gutmann JL, Gao Y: Alteration in the inherent metallic and surface properties of nickel-titanium root nickel root canal instruments enhance performance, durability and safety: a focused review, Int Endod J 45:2, pp. 113-128, 2012.
11. Metzger Z, Teperovich E, Zary R, Cohen R, Hof R: The self-adjusting file (SAF). Part 1: respecting the root canal anatomy—a new concept of endodontic files and its implementation, J Endod 36:4, pp. 679-690, 2010.
12. Yared G: Canal preparation using only one Ni-Ti rotary instrument: preliminary observations, Int Endod J 41:4, pp. 339-344, 2008.
13. Hashem AA, Ghoneim AG, Lutfy RA, Foda MY, Omar GA: Geometric analysis of root canals prepared by four rotary NiTi shaping systems, J Endod, 38:7, pp. 996-1000, 2012.
14. Blum JY, Machtou P, Ruddle CJ, Micallef JP: Analysis of mechanical preparations in extracted teeth using the ProTaper rotary instruments: value of the safety quotient, J Endod 29:9, pp. 567-575, 2003.
15. West JD: The endodontic glidepath: secret to rotary safety, Dent Today 29:9, pp. 86, 88, 90-93, 2010.
16. Dentsply International, personal communication.
17. Johnson E, Lloyd A, Kuttler S, Namerow K: Comparison between a novel nickel-titanium alloy and 508 nitinol on the cyclic fatigue life of ProFile 25/.04 rotary instruments, J Endod 34:11, pp. 1406-1409,
This article was taken from the official Dentsply Sirona resource https://www.dentsplysirona.com/