Summary
Breakage of nickel-titanium instruments is a major problem in endodontic treatment. A study examining the failure of nickel-titanium files due to torsional loading found that the majority of such failures occurred at the tip of the tool within the last millimeter and in instruments that had a small taper and/or size. Consequently, the tip of small instruments is at higher risk of breakage due to torsional loading, and to prevent this, the use of torque-reducing motors is necessary to reduce apical pressure and prevent the instrument tip from becoming stuck in the root dentin. In contrast, flexural fracture occurs as a result of repeated subthreshold loading resulting in metal fatigue. Numerous studies examining the causes of overload and breakage of machine-assisted nickel-titanium files have confirmed that by pre-expanding the root canal using hand instruments and creating a glide path before using machine instruments, a significant reduction in the rate of breakage can be achieved. This fact highlights the importance of manually pre-expanding the root canal and creating a “glide path” to reduce the incidence of mechanical instrument failure. To pre-expand the root canal and create a “carpet path,” hand-held steel instruments are most often used. Unfortunately, they have a number of disadvantages due to their relative rigidity and the presence of an aggressive tip, which can lead to the formation of ledges or changes in the course of the root canal in curved and/or calcified canals. For this reason, a new PathFile™ (Dentsply Maillefer) set for glide path creation and root canal pre-expansion was recently introduced, consisting of three machine-made nickel-titanium instruments.
PathFile™ are the first instruments specifically designed and intended for the mechanical creation of carpet and pre-enlargement of the root canal. The combination of a low 2% taper, a square cross-section and 4 cutting edges makes these instruments highly flexible, durable and effective, enabling fast and safe treatment of even severely curved and/or calcified root canals. Preliminary scientific research and clinical trials have confirmed that PathFile™ instruments are highly effective in treating severely curved root canals, allowing the creation of a perfect “glide path” without altering the course of the root canal, even if the working length is incorrectly determined.
Reciprocating tip
In 1964, the Giromatic system was introduced for mechanical treatment of root canals. The system was developed to save time on canal processing and is currently represented by a contra-angle handpiece with special files resembling pulp extractors (Ripsi file) or having a screw shape (Hele file). The constant rotation in the tip is transformed into another - a quarter turn movement. In some tips, reciprocating movements in the vertical direction of 0.8 - 1 mm (Endo - Cursor) are carried out every quarter turn.
The poor clinical outcome of these techniques may have been due to the inadequate design of the endodontic instruments used. In the 1980s, these problems were overcome with the development of "Dynatrat" files, S-shaped files with a smooth tip without grooves (guide tip only). They were used to process the coronal 2/3 of the canal, and then the apical third was processed manually.
It should be noted that many works have appeared comparing manual and machine processing of canals. It was noted that during machine processing, especially in curved canals, the canal very often acquired an “hourglass” shape. In addition, the problem arose of clearing the channel from sawdust, and the constant threat of blocking the channel with it. Gaining time in preparation turned into losing time in cleaning the canal. The time required was comparable to or even greater than manual preparation. Losing the “channel sense” led to complications.
Introduction
The use of machine-made nickel-titanium instruments has radically changed the technique of mechanical root canal preparation and the prognosis in difficult clinical situations. Numerous “invitro”1−13 and “invivo”14−17 studies have shown that machine-made nickel-titanium instruments are superior to steel hand files in the quality of root canal formation and the possibility of their use in canals with pronounced curvature, reducing the risk of creating ledges or straightening the canal curvature . Schäfer16 conducted an in vivo study in which 110 root canals were treated with machine nickel-titanium instruments and 84 canals with hand instruments. All canals were processed by 8 experienced doctors. Before the start of treatment and after obturation of the canals, x-rays of each tooth were taken.
Straightening the curvature. Nickel-titanium machine tools.
Work time. Manual steel files.
Rice. 1. Probability of root canal straightening and working time after in vivo root canal debridement using nickel titanium machine tools and hand steel files (adapted from Schäfer et al.16).
Straightening of the root canal curvature was assessed using a computer image analysis program. Root canal preparation using machine-assisted nickel-titanium instruments significantly reduced working time and resulted in less straightening of the canal curvature compared to the use of hand instruments16 (Fig. 1). In another in vivo study, Sonntag et al17 compared the risk of complications in root canal preparation with hand-held steel instruments and machine-operated nickel-titanium instruments. All clinical cases were performed by students. The results demonstrated that even in the absence of sufficient experience on the part of the practitioner, the quality of root canal preparation using nickel-titanium instruments was higher than that using manual steel files, while the number of shoulders was significantly reduced and the integrity of the apical foramen was maintained.17 Unfortunately, the use machine-made nickel-titanium instruments have serious limitations as they are associated with an increased likelihood of file breakage within the canal compared with steel instruments.17,18 Suter et al. When assessing in vivo the possibility of successfully removing a broken instrument from a root canal, success rates are reported to be 87% of cases. Studies of removed instrument fragments confirm that machine-made nickel-titanium instruments break more frequently than hand-operated steel instruments.18 Sonntag et al.16 report that breakage of nickel-titanium instruments is a major problem in endodontic treatment. Studies evaluating the influence of various factors on the breakage of machine endodontic nickel-titanium instruments have demonstrated that file breakage occurs primarily under the influence of torsional load19−25 and instrument fatigue.21,23,26−28 Torsional load depends on the contact area of the instrument with root canal dentin, the taper and diameter of the instrument, the area of the instrument subjected to stress, the strength (cross-sectional shape) of the instrument, the design of the working part, and the torsional load applied to the instrument.27,28 A study on the failure of nickel-titanium files due to torsional load has shown that the majority of such failures occur at the tip of the tool within the last millimeter and for instruments that have a small taper and/or size.24,25,27,28 Consequently, the tip of small-sized instruments is at higher risk of failure due to torsional loading, and to prevent this, the use of torque-reducing motors is necessary to reduce apical pressure and prevent the instrument tip from becoming stuck in the root dentin.27,28 In contrast, flexural fracture occurs as a result of repeated subthreshold loading, resulting in metal fatigue.
The bending load depends on the radius of curvature and size of the root canal, the rotational speed and flexibility of the instrument, the characteristics of the nickel-titanium alloy, the presence of intracanal obstructions, and sudden changes in the course of the root canal (for example, in the case of fusion of canals or the presence of additional canals).27,28 Numerous Studies examining the causes of overloading and failure of machine-assisted nickel-titanium instruments have confirmed that a significant reduction in the incidence of machine instrumentation failure can be achieved by pre-enlarging the root canal using hand files and creating a “glide path” before using machine instruments. In a study of the effect of pre-enlargement of the root canal on the failure rate of 4% taper nickel-titanium machine instruments, Roland et al.29 concluded that “pre-enlargement of the root canal with hand files followed by the use of machine instruments allows the instruments to be used more times before failure than with the isolated use of the crown down technique recommended by the manufacturer.” Peters et al.,30 examining the physical performance of machined nickel-titanium ProTaper instruments in the treatment of curved maxillary molar canals “in vitro”, showed that “even when significant load was applied in some clinical cases, no ProTaper instrument failed in the presence of adequate "carpet path" Blum et al.31, after analyzing the mechanical preparation of extracted teeth using ProTaper machine instruments, determined that “particular attention in a precise root canal protocol should be given to the use of small, flexible hand-held steel files to ensure that each part of the root canal has sufficient space for unobstructed machine access.” tools in the process of further machining...". Berutti et al32 evaluated the effect of manual root canal pre-expansion and torque on failure rates using ProTaper machine instruments. In this study, the authors used 400 plastic training blocks divided into 2 groups. All blocks were processed with ProTaper instruments, but one group had the canal pre-dilated manually using hand instruments to ISO #20 before using machine files. The results of the study showed that after manually pre-expanding the root canal, ProTaper instruments were able to process significantly more plastic blocks before failure occurred32 (Figure 2).
Rice. 2.
Number of plastic training blocks processed to failure by ProTaper S1, without pre-expanding the canal to a #20 ISO file and with pre-expansion. Adapted from Berutti et al.32 No pre-expansion. Pre-extension to ISO file #20.
Finally, Varela et al33 examined the effect of manual canal pre-expansion on the failure rate of three different nickel-titanium machine instruments (ProFile, ProTaper and K3) when used in canals of extracted teeth with curvature greater than 30º. The authors demonstrated a significant reduction in the incidence of file breakage when performing preliminary manual root canal expansion before using machine instruments. In this study, there were no significant differences between the three types of instruments used.33 All of the above studies suggest that the beneficial effect of pre-manual reaming is to reduce the likelihood of the tip of the weakest instruments becoming stuck in the root canal.28−33 In addition, As an explanation for the reduction in machine instrument failure in curved root canals, not only the presence of a smooth “carpet path” to prevent dangerous deformation of the instrument tip must be taken into account, but also the reduction in bending load.28,30,32
Preliminary enlargement of the root canal and creation of a “carpet path” is most often carried out using manual steel files. Unfortunately, these instruments have a number of disadvantages due to their relative rigidity and the presence of an aggressive tip, which in curved and/or calcified canals can lead to the formation of a shoulder or change in the course of the root canal.34 For this reason, the new PathFile™ set was recently introduced (Dentsply Maillefer) for creating a “carpet path” and preliminary expansion of the root canal, consisting of three machine-made nickel-titanium instruments.
Rice. 3.
PathFile™ No. 1−3 (Dentsply Maillefer). PathFile™ No. 1 (0.13 mm). PathFile™ No. 2 (0.16 mm). PathFile™ No. 3 (0.19 mm).
Experience in using hand instruments to prepare root canals for obturation
It is known that the success of endodontic treatment depends on how thoroughly the intracanal tooth system was cleaned, developed and disinfected [1, 3, 5]. The functional durability of the tooth is determined, in turn, by the quality of the hermetic and three-dimensional filling of the root canal (RC) with filling material. According to some authors, errors in the treatment of apical periodontitis are the most common cause of loss of functional teeth in young and middle age (Sinitsa V.V. et al., 2000; Beer R., 2002; Lukinykh L.M., Livshits Yu. N., 2004).
Preparing a CC for filling (preparation) requires the dentist to have certain work experience and good manual skills. As the luminaries of endodontics say, in order to learn how to confidently and predictably prepare a CC for obturation, you need to develop dozens of meters of canals with manual files, that is, by hand. Only with the development of treatment experience does a special tactile sensitivity of the fingers arise when working with files in the canal [2, 4, 8, 11].
It is our deep conviction that every dentist who deals with canal treatment must have manual skills in working with hand-held endocanal instruments in order to prevent a threat to the patient’s health. Thus, according to some data, up to 39% of odontogenic inflammatory processes in the maxillofacial area are the result of illiterate actions of a dentist in the treatment of apical periodontitis (Bazhanov N. N. et al., 1997).
In the distant pre-perestroika time, our country had a mentoring system. An experienced doctor was assigned to the young specialist, who supervised the work of the young doctor, helped in his work and contributed to his professional growth.
By the way, the mentor was asked quite strictly about the quality of the young specialist’s training! Currently, after graduating from an educational institution, doctors are left to their own devices and everyone works as best they can, and the result is a cemetery of extracted teeth that could have functioned for a long time if assistance at the stage of canal preparation had been provided in a qualified manner [1—3, 7, 11] .
It is the unprofessional treatment of canals for periodontitis, according to some authors, that is the cause of the development of periostitis of the jaws in at least 65% of patients, osteomyelitis in 75% of patients, and phlegmon of the maxillofacial area in 69% of patients (Maksimovsky Yu. M., Grinin V. M., 2004).
It is very sad that currently only 15-20% of doctors are active in acquiring knowledge, reading, studying at various seminars and conferences and implementing the acquired knowledge and advanced techniques into practice.
The importance of the problem of high-quality preparation of CC for filling also lies in the fact that the doctor’s errors and shortcomings at the stage of preparation and obturation of the canal contribute to the further chronicization of the process in the periapical tissues and the emergence of odontogenic formations [1, 3, 7, 13]. At the same time, successful preparation of CCs and their high-quality three-dimensional obturation contributes to the reverse development of periapical lesions of odontogenic origin (Borovsky E.V., et al., 2002; Lukinykh L.M., Livshits Yu.N., 2004; Yudina N. A. et al., 2006).
It is very sad that (according to Prof. V.V. Boyko) currently only 15-20% of doctors are active in acquiring knowledge, read, study at various seminars and conferences and implement acquired knowledge and advanced techniques into practice [7]. The results of a survey conducted on the basis of the Department of Dentistry of the Faculty of Postgraduate Education of St. State Medical Academy of dentists working in the compulsory medical insurance system on endodontic issues are interesting [11].
Thus, only 7.9% of dentists use apex locators, 2.3% know and use average tabular data on the length of tooth roots, 43.8% use instruments with silicone length limiters and 3.6% use a ruler to determine the working length of the root channel.
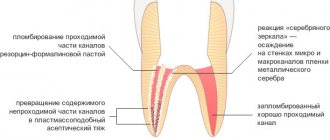
The possibility of using phosphate cement for obturation of root canals was indicated by 22.3% of respondents, 67.4% of doctors regularly use the resorcinol-formalin method, only 3.5% of doctors used materials based on calcium hydroxide. Up to 70.5% of doctors neglect X-ray examination before treatment, 78.9% during treatment, 45.4% after root canal filling.
Thus, the lack of information about modern technologies and manual skills in root canal treatment, on the one hand, and the immaturity and reluctance of doctors to improve their professional level, on the other hand, are a consequence of a large number of complications after endodontic dental treatment [3, 7, 9, 13].
The purpose of this article is to share with novice clinicians clinical experience in cleaning and preparing CCs for obturation using hand endodontic instruments. Currently, dentists, including us, widely use various mechanical (rotary) and vibration endodontic systems to facilitate and speed up the preparation of the oral cavity for obturation, but not a single system can do without the use of hand instruments! Whether it is a rotary or the most advanced reciprocal rotation system (Dr. Ghassan Yared, 2012), curved, obliterated and other problematic canals require the use of hand instruments. That is why every doctor working with CC must have skills in working with hand tools.
Modern endodontic instruments are manufactured using the latest scientific developments and high technologies [6, 10, 12]. Currently, leading companies provide a large selection of high-quality instruments for the preparation of CC. With all the wide choice of endodontic instruments, the main ones are K-files and H-files. Many instruments are used for specific indications (slit-shaped canal, curvature, destruction, etc.) and are therefore less in demand. They differ from each other mainly in the composition of the metal and the nature of the cutting surface [9, 11, 12].
K-files (the initial letter stands for the first manufacturer of the instrument, Kerr), in turn, are divided into K-files and reamers. In our practice, we prefer to work with reamers, which differ from K-files in the number of turns per 1 mm (0.80-0.28) and are designated by a triangle. K-files with a number of turns of 1.97–0.88 per 1 mm are more aggressive and are indicated by a rectangle at the end of the tool [4, 6, 9, 12].
With all the wide choice of endodontic instruments, the main ones are K-files and H-files. Many instruments are used for specific indications (slit-shaped canal, curvature, destruction, etc.) and are therefore less in demand.
But both tools are durable and reliable when processing any direct QC. When working in the movement channel there must be filing. In our practice, we prefer to combine the reciprocating movements of the reamer with turning half a turn clockwise and half a turn counterclockwise, which prevents the instrument from jamming in the canal and pushing dentinal filings beyond the apex.
The H-file (Headström) is a very aggressive tool due to the fact that the helix angle is close to 90 degrees relative to the central axis. It is used to clean straight and wide CCs from gangrenous pulp residues and decay through reciprocating movements. Rotation of the tool around its axis is prohibited due to the high probability of jamming and breaking off the top of the tool.
K-Flexorimer (from English Flex: bend, bend) is an instrument with increased flexibility for the preparation of curved CCs and should be used through a reciprocating motion (up and down).
K-Flexorimer golden medium is used during preparation to safely transition from one instrument size to another, to prevent the formation of ledges and jamming.
K-file nitiflex (Maillifer) is made of a nickel titanium alloy with a non-corrosive tip and increased flexibility and durability and is designed for the preparation of highly curved and narrow canals.
The Pathfinder is made of high quality stainless steel and has an aggressive tip, minimal taper, tapered spiral edges and sufficient flexibility, thereby allowing the preparation of narrowed and obliterated CCs.
Pathfinder CS (Kerr) is made of carbon steel, which gives it additional high strength and ensures its use in sclerotic CCs.
K-Reamer Farside (Maillifer) - reamers of reduced length (15-18 mm) and small diameter (06, 08, 10 and 15 according to the ISO standard), designed for the initial expansion of narrow oral cavity with limited mouth opening (chewing teeth, wisdom teeth, lockjaw).
K-Reamer Deepstar (Maillifer) is a set of shortened K-Reamers (15 and 18 mm) with a sharp aggressive tip, designed for unsealing K-Reamers.
K-Flex Options (Kerr) - with a non-aggressive tip, provides increased flexibility. Used when working in highly curved CCs.
The Apical Reamer has a non-aggressive tip and is threaded only on the top third of the tool. Used for preparation (finishing) of the apical part or for strongly curved CCs.
There are several ways to process CC [4, 9, 12]. However, they all have a common goal: the final shape of the prepared canal must have a funnel-shaped and continuous expansion from the apex to the mouth (carrot). This helps ensure irrigation of the canal, its disinfection and further three-dimensional obturation.
In working with QC, several successive stages can be distinguished. Thus, at the initial stage it is necessary to determine the working length radiographically or electronometrically. Then, if possible, carry out the initial cleaning of the contents of the CC (pulp, remains of necrotic tissue, calcification, etc.). After this, there will be direct work in the QC, which is also divided into three stages. Conventionally, the CC is divided into three components: the coronal (estuarine) third, the middle third and the apical third. Depending on the individual characteristics of the CC system and the clinical situation, the doctor begins work using one of the generally accepted methods - from crown to apex (CROWN-DOWN) or from apex to the mouth of the crown (STEP BECK) [4, 5, 9, 12].
There are several ways to process QC. However, they all have a common goal: the final shape of the prepared canal must have a funnel-shaped and continuous expansion from the apex to the mouth (carrot).
CROWN-DOWN - from crown to apex - involves the initial expansion of the mouth third of the CC using Gates Glidden, Largo or Butelrock Reamer. Then, step by step from the crown, we evacuate the contents of the canal using hand tools in descending order. Moving to the apical third of the canal, the movements of the fingers with the instrument become more careful and delicate, combining the advancement of the instrument to the apex with elements of rotating the file clockwise and counterclockwise.
It is mandatory to use abundant irrigation after each removal of the instrument to remove dentinal filings. Currently, sodium hypochlorite (NaOCl) is the most effective irrigation solution available, although it does not remove the smear layer inside the canal. The advantage of this technique, with due care and caution of the doctor, is that there is no danger of pushing the infected contents past the apex. The indications for the use of this technique are very wide, but the use actually depends on the preferences of the doctor and some minor restrictions.
STEP BECK is a reverse preparation technique, i.e. from the root apex to the crown. The work begins with leasing (carpet) with K-file 010 and determining the working length using an apex locator or dental radiograph. First, the thinnest instrument (H-file) cleanses the lumen of the coronary artery from residual pulp and infected contents.
Then comes the sequential preparation of the apical third: the principle from smallest to largest is observed. Most often, in the apical region, we work to the full working length up to an ISO 025 instrument, using copious irrigation of sodium hypochlorite. After 025 of the tool, the next file (030) is immersed into the channel to a depth less than the working length by 1 mm, the next one (035) by another 1 mm, and so on like a telescopic fishing rod, including the middle third in the process to the required size.
Any system involves the use of endodontic lubricants based on EDTA, which dissolves the smear layer that forms on the canal walls after the use of hand instruments, and is a kind of lubricant for advancing the file. Preparations for chemical expansion of canals (endolubricants) based on EDTA are used in the form of solutions and gels.
The first group includes “Largal ultra” (Septodont), “Edetal solution” (Pierre Rolland), “Liquid for chemical expansion of root canals” (“Omega Dent”), etc. The group of EDTA-based gels includes “Canal +” ( Septodont), "RC-prep" (Premier), "Edetal" (Omega Dent), etc. Today, the most effective method for removing organic substrates and the smear layer is the use of EDTA-based endolubricants in combination with sodium hypochlorite [5, 7, 9, 12].
Due to the fact that the cross-sectional shape of CC has great variability: round, semicircular, irregular, oblong, dumbbell-shaped, oval, triangular, their preparation requires an individual approach [11].
Depending on the initial situation, you have to vary, choosing between one or another QC instrumentation technique, and even combine them. However, in any case, all attention is focused on the tip of the file! When moving a file into the CC, the resistance of the file, signs of jamming or, conversely, the absence of any resistance, viscosity, bleeding and other factors are taken into account. Each sign characterizes a certain condition in the CC and requires certain actions by the doctor.
Due to the fact that the cross-sectional shape of CC has great variability: round, semicircular, irregular, oblong, dumbbell-shaped, oval, triangular, their preparation requires an individual approach.
Resistance when advancing the file indicates destruction of the CC, curvature, and narrowing. At the same time, the absence of resistance indicates either the initial stage of the inflammatory process in the pulp, unformed roots, or a long-term inflammatory process with the phenomena of resorption of the root apex and periapical changes. In this case, under the control of dental radiography with a file inserted into the canal or a visiograph, a thicker initial file is selected and the preparation is carried out according to one of the existing methods.
Viscosity when moving the tool into the CC. You have to put some effort into moving the file. This picture is typical when filling KK with pastes (resorcinol-formalin, eugenol-zinc) or root cements (paracin-cement, Ovrutsky’s cebanite, Antonova’s zincoplast, intradont, etc.).
In this case, it is appropriate to use the Pathfinder instrument, which has an aggressive tip, sharpened spiral edges and sufficient flexibility, which allows the preparation of narrowed and obliterated CCs. Then you can connect the H-file (Hedstrom). In this case, special preparations are used [4, 5, 9, 12] to soften root fillings based on phenoplast (resorcinol-formalin) resin “Endosolv R” (Septodont), “Resosolv” (Pierre Rolland), “Solvadent-gel” VladMiVa ), "Phenoplast" ("Omega Dent"), etc. To soften filling materials that contain eugenates, "Endosolv E" (Septodont), "Solvadent-gel" ("VladMiVa"), "Evgenat" (" Omega Dent"), etc.
Bleeding from the CC indicates the presence of residual root pulp or perforation. To stop bleeding from the CC, a 3% aqueous solution of hydrogen peroxide or a 0.5-1.0% solution of sodium hypochlorite is used, which are injected into the canal on a paper absorber. You can use a 5% solution of aminocaproic acid, a 1% solution of adrenaline, liquid phosphate cement or calmecin powder [5, 8]. You can connect diathermocoagulation of the channel. But first of all, it is necessary to determine where the bleeding is coming from.
A sign of perforation is heavy bleeding from the CC, which resembles arterial bleeding! In this case, we should think about whether we are moving in the right direction and whether we are in the channel! A control dental radiograph with an instrument will clarify the picture. Then, under X-ray control, it is necessary to correct the direction of the file (reamer, Pathfinder) and continue the preparation of the CC. Subsequently, the perforation area is closed with “ProRoot” MTA (Dentsply) and the CC is sealed.
Tool jamming. Depending on the depth of promotion, certain tactics are required. So, if jamming occurs in the middle third of the valve, then this is either a narrowing, or curvature, or a previously filled valve. In this case, the doctor’s actions are aimed at expanding this area, starting with a smaller instrument (K-file nitiflex Pathfinder CS, K-Flex Options) using EDTA. The movements should be reciprocating with clockwise rotation half a turn and counterclockwise, you must first dip the tool in EDTA gel. If necessary, the instrument is bent according to the curvature of the canal.
If jamming occurs in the apical region, indicating a sharp root bend, narrowing or step, care should be taken to break off the tip of the instrument. Therefore, the movements should be soft and careful with elements of the balanced force technique, i.e., moving the file (Apical Reamer) to the apex, scrolling it counterclockwise. When preparing, the instrument must be curved according to the curvature of the canal. In this case, in addition to endolubricants, copious irrigation of sodium hypochlorite should be present.
At the initial appointment, if you are faced with problematic canals that cannot open (destruction, sclerosis, or previously filled), you should not try to open them on the first visit.
Having worked with channels for a long time, we have compiled recommendations that may be useful for novice doctors.
First of all, it is impossible not to cite the statement of one experienced doctor who defines the concept of working with canals. Experience is an interesting thing. Over time, the doctor did not learn to better navigate obliterated canals with fragments of broken instruments, but he learned to understand where to go and where not to go [13].
At the initial appointment, if you are faced with problematic canals that cannot open (destruction, sclerosis, or previously filled), you should not try to open them on the first visit. First, we dissect the opened CCs, and leave the intractable ones for the next visit! After all, most doctors are tied to patient registration and queues for appointments, so they do not have enough time to fully prepare the canals.
You cannot disrupt the sequence of QC development with files! That is, despite the apparent ease of the opened CC, jumping from one file number to another through one or more is fraught with blocking the CC lumen, jamming the file, breaking off its tip and getting a problem that requires much more effort and time than you wanted to save by breaking sequence of operations.
Contrary to the recommendations to move the file only up and down, we, moving the reamer to the apex of the root, slightly scroll it left and right and, having reached a certain resistance, release it from the canal. We prefer to work more, turning the reamer slightly counterclockwise: according to Ioffe - the balanced force method - but not purely according to his recommendations. These precautions are especially important when unfilling CVs and destructive periodontitis.
Before moving on to a thicker file, we perform reciprocating filing movements with scrolling clockwise and counterclockwise. K-Flexorimer golden medium intermediate tools are used for the same purposes. The feeling of ease of moving the instrument in the canal indicates the possibility of using a file of the next size.
In your work, you should not adhere to only one concept, one treatment tactic, one author (from whom the doctor was once trained). It is more correct to evaluate the clinical situation in each specific case and try to adapt an acceptable method or technique or a combination of both to it. Don't bow to authority!
Analyze the results of your work and failures, long-term results. During the initial examination of the next patient, pay attention to the work performed by other doctors, comparing your skills and achievements, thus, as if adopting the positive experience of colleagues.
When faced with a problematic situation at an appointment, do not rush to solve the problem yourself by any means. It is better to reschedule the appointment and seek advice from more experienced colleagues, including communication via the Internet. And at the next appointment, armed with knowledge, calmly solve the complex problem that has arisen. Thus, you will observe the main commandment of the doctor: “Do no harm.”
The patient is always right! This axiom is applicable to the entire service sector, including dental appointments. Memories are still fresh of a case in pre-perestroika times, when, in response to a patient’s complaints about tooth pain, the dentist categorically stated that the tooth was intact and the woman was simply making things up and being harmful...
When faced with a problematic situation at an appointment, do not rush to solve the problem yourself by any means. It is better to reschedule the appointment and seek advice from more experienced colleagues, including communication via the Internet.
Now we know that the patient was probably right and there may be plenty of reasons to complain about an apparently healthy tooth. I would like to protect novice doctors from such statements. After all, unlike a cosmetology office, hardly anyone will go to a dentist’s office without proper motivation. It is our deep conviction that we must trust patients, be able to listen to them and, quietly guiding the conversation in the right direction, collect a complete medical history to make the correct diagnosis.
Thus, the quality of CC preparation for complicated caries depends on the doctor’s professionalism, which is developed through participation in scientific conferences, seminars, reading specialized literature and communicating with senior colleagues. At the same time, having developed certain manual skills in preparing canals with hand tools, you can guarantee in advance a good predictable result when working with canals of any cross-sectional shape. Knowing the purpose and indications for the use of modern hand endodontic instruments, you can achieve success in preparing the canal for permanent obturation much faster and with less labor.
LITERATURE
- Aksenova T.V., Napolnikov L.V., Grechishnikov V.V. Rehabilitation of periapical tissues in chronic apical periodontitis: main directions and methods //Kuban. scientific medical messenger - 2002, No. 4(61). — P. 4-6.
- Borovsky E.V. Treatment of complications of dental caries: problems and their solutions // Dentistry. - 1999, No. 1. - P. 21-24.
- Dmitrieva L. A., Selezneva T. V. New trends in the treatment of apical periodontitis // Endodontics today. - 2004, No. 1-2. — P. 30-31.
- Joffe E. Moving with caution along the path of progress // Dental South. - 2007, No. 45. - P. 24-26.
- Kozlov V. A. Dentistry. - St. Petersburg, 2003. - P. 164-174, 197-207.
- Krammer I., Schlepper H. Guide to endodontics. - M.: 2000. - P. 44-46.
- Maksimova O. P. Two sides of endodontics // Clinical dentistry. — 2012, No. 1 (61). — P. 32-34.
- Malanyin I.V., Pavlovich O.A. Guide to pharmacology in endodontics. - Krasnodar, 2006. - pp. 54-58.
- Malanyin I.V. Clinical periodontology. - Krasnodar, 2006. - pp. 291-300.
- Malanyin I.V., Pavlovich O.A. Materials science in endodontics. - Krasnodar, 2008. - pp. 56-58.
- Sirak S.V., Shapovalova I.A., Kopylova I.A. Complications arising at the stage of filling the root canals of teeth, their prediction and prevention //Endodontics today. - 2009, No. 1. - M.: POLY MEDIA PRESS. — P. 23-25.
- Stephen Cohen, Richard Burns. Endodontics. - St. Petersburg: Peace and Family - 95, Interline, 2000. - P. 169-171.
- Sumelidi A.P. Endodontics in Russian //Dental South. — 2009, No. 3 (63). - pp. 14-16.
PathFile™ Tools Sequence
The sequence of using PathFile™ tools is very simple (Fig. 4):
1 – Primary navigation and examination of the root canal with a K-file No. 10, which should freely enter the canal to the working length. To speed up this stage, if necessary, use endolubricants containing EDTA.
2 – Determination of working length using an electronic apex locator and (or) radiography.
3 – Pass PathFile™ No. 1 (0.13 mm) to working length.
4 – Pass PathFile™ No. 2 (0.16 mm) to working length.
5 – Pass PathFile™ No. 3 (0.19 mm) to working length.
6 – You can then begin using the nickel titanium files using standard techniques (if using the ProTaper system, use file S1).
PathFile™ are used in a gentle reciprocating motion at 300 rpm, motor torque of approximately 5 Ncm until full working length is reached. Significant apical loading on instruments should be avoided. The use of relatively high motor torque is not harmful given the square cross-section of the tool and the results of a study by Berutti et al.38 which demonstrates that the use of high torque allows nickel-titanium machine tools to machine significantly more channels before failure.38 The time required to work with three PathFile™ files per working length does not exceed 3 – 5 seconds for each tool; increasing the working time is useless, but not dangerous, since PathFile™, thanks to their high flexibility, do not change the course of the canal even in the event of errors in determining the working length. Copious irrigation is recommended after each instrument, although PathFile™ coils do not become clogged with dentinal filings and these instruments do not cause filing blockage of the apical foramen.
Rice. 4.
Sequence of using PathFile™ tools. X-ray before treatment (4A). Determination of the working length of the palatal and medial buccal 1 canals (4D). Radiograph showing the master pin in the medial buccal 1 and medial buccal 2 (4E), and in the distal and palatal canals (4F). X-ray immediately after treatment (4G) and 1 year later (4H).