How does it manifest?
Doctors identify the following clinical symptoms that appear in a victim with a throat burn:
- Sharp pain in the throat, with a tendency to intensify when trying to swallow;
- Intense salivation;
- Nausea and vomiting;
- Cough syndrome;
- Pain localized in the chest area;
- Voice changes;
- Feeling of lack of air;
- Swelling of the cervical lymph nodes;
- A strong burning sensation in the palate;
- Hiccups.
In severe cases, a state of shock may develop. Even minor injuries can cause respiratory problems and cause suffocation, especially when it comes to a child or an elderly person.
Therefore, having identified the first symptoms characteristic of this injury, you should urgently provide first aid to the victim, then take him to a medical facility and transfer him to the hands of professionals.
Possible consequences
With this injury, patients are highly likely to develop complications and adverse consequences, which include:
- Chemical intoxication, poisoning;
- Collapse;
- Reflex cessation of breathing associated with damage to nerve endings;
- Scarring of the larynx, pharynx and esophagus area.
Causes of the pathological process
Burns occur accidentally or intentionally. The main reasons for the development of this pathology are :
- Failure to comply with industrial safety regulations. In this case, ingestion of chemicals or inhalation of hot steam may occur;
- Consumption of strong alcoholic drinks, pure alcohol;
- Treatment of the throat mucosa with iodine and drugs based on it. Such drugs are used for sore throat and pharyngitis. But quite often a chemical burn occurs;
- Eating hot food. This is often observed in young children;
- Accidental use of chemicals. It is observed in young children who taste everything. This reason is also relevant for alcohol abusers, who may confuse the chemical with an alcoholic drink;
- Drinking excessively hot drinks (such as tea);
- Consumption of acids or alkalis for the purpose of suicide.
Read also: Why do your hands shake a lot?
Pre-hospital care measures
What to do if the larynx is burned? First of all, it is recommended to give the victim a drink of cold water, which will alleviate the general condition, relieve pain and swelling, but most importantly, prevent further spread of the burn into the depths of the tissue.
In this case, you need to drink water in small sips, holding it in the throat and mouth. A good effect is obtained by sucking crushed ice or rinsing the larynx with cool antiseptic solutions. In case of a chemical burn, it is necessary to neutralize the effect of the provoking factor. For these purposes, you need to examine the victim’s larynx.
With an alkaline lesion, a dry scab will be noticeable on the mucous membranes. In this situation, a weak solution of acetic or citric acid is used. If a jelly-like scab forms in the throat, then we are talking about exposure to acids, and the patient needs a soda solution to neutralize it.
After providing first aid and alleviating acute symptoms, you need to give the victim a gastric lavage, give him a glass of milk and a little sunflower oil, and then be sure to contact a specialist who will prescribe further treatment!
A burn of the mucous membrane of the throat of the first degree and sometimes the second is treated at home; in more severe cases, the victim is hospitalized. Successful treatment and recovery requires compliance with the following medical recommendations:
- Silence. The patient should talk as little as possible and avoid raising his voice.
- Rinse with chamomile decoction and antiseptic solutions.
- Abstinence from spicy, sour, hard salty foods.
- Following a diet with a predominance of liquid and puree foods. The patient's menu should include broth, sour cream, cheese, eggs.
- Throat burn: symptoms, first aid and treatment
For burn lesions of the throat, treatment involves mandatory drug therapy. A qualified specialist will advise you individually on how to treat a lesion in a particular case. Patients are usually prescribed analgesic and antibacterial drugs, and glucocorticosteroids are used to reduce swelling.
The mucous membranes of the larynx in the affected area are regularly treated with antiseptic and oil products - such procedures give a very good therapeutic effect! The surface of the larynx can also be lubricated with Vaseline, beaten chicken egg, using a sterile cotton swab.
Among the most common traditional medicines used to combat this disease are the use of peach, olive, sea buckthorn and rosehip oils. These products can be used for oil inhalations and external treatment of burned areas. Home treatment for thermal burns may include oil inhalations, sucking ice cubes, applying cold neck compresses, rinsing with sage and chamomile infusions.
Proper recovery also requires certain diet therapy. Products such as egg whites, vegetable and butter, cool drinks, and cream contribute to the speedy rehabilitation of the patient. For medicinal purposes, the oil is consumed in its pure form, 4 times a day.
The role of alcohol abuse in esophageal damage
Surgical department No. 2 (city center for gastroduodenal bleeding of ulcerative etiology), surgeon Konkin D.K.
For a long time, gastroenterologists paid undeservedly little attention to the esophagus. The reason for this was largely that the esophagus is the only organ of the digestive system that is not subject to physical examination: it cannot be palpated, percussed, or auscultated. And only in the 70–80s of the last century, with the advent and widespread use of endoscopic examination, interest in the pathology of the esophagus increased significantly. The International Society for Diseases of the Esophagus (ISDE) is currently active. Basic and clinical research is constantly being conducted to study the pathology of the esophagus. Thus, diseases of the esophagus are very relevant in world gastroenterology.
On the other hand, an equally pressing problem of modern medicine is pathological conditions associated with alcohol abuse. It has long been known that alcohol, when consumed systematically, can lead to diverse damage to various organs and systems of the body. Of course, alcohol has a significant pathogenic effect on the digestive system, since it is the first to come into contact with ethanol. Among the main pathogenic effects of alcoholic beverages on the gastrointestinal tract, the following should be noted: increased gastric secretion, slower gastric evacuation function, impaired absorption of nutrients in the small intestine, increased transport of toxins through the intestinal wall, impaired intestinal motility with a tendency to diarrhea, and others.
What is the effect of alcohol on the structure and function of the esophagus? The pathogenic effect of alcohol consumption on the esophagus is multifaceted, both in the nature and severity of the lesions.
Considering the known toxic properties of alcohol and the fact that almost the first organ with which alcohol comes into contact is the esophagus, it is logical to assume a direct toxic effect of ethanol on the esophageal mucosa. Indeed, prolonged contact of ethanol with the mucous membrane of the esophagus can lead to the development of alcoholic esophagitis. The development of alcoholic esophagitis can be caused not only by the toxic effect of alcohol, but also by a decrease in the secretion of the salivary glands with prolonged alcohol abuse, which has protective properties for the esophageal mucosa.
Another important area of the pathogenic effect of ethyl alcohol on the esophagus is a violation of its motility. Some patients who abuse alcohol have difficulty swallowing, which may be clinically accompanied by dysphagia. A more common effect of alcohol on esophageal motility is disruption of the normal functioning of the lower esophageal sphincter. Insufficiency of this sphincter is often observed, which can lead to the development of gastroesophageal reflux disease (GERD). However, in patients who abuse alcohol for a long time, the opposite disorder is possible - increased tone of the lower esophageal sphincter. Another common and important disorder of the motor function of the esophagus is decreased peristalsis. Decreased esophageal clearance is an important prerequisite for the development of GERD.
As already mentioned, alcohol consumption is associated with an increased development of such a common pathology as GERD. As is known, GERD is a chronic recurrent disease, manifested by the development of characteristic symptoms (heartburn and others) and the development of inflammatory and erosive lesions of the distal parts of the esophagus due to regular reflux of gastric or duodenal contents into the esophagus. Indeed, for many people, even occasional consumption of alcoholic beverages is accompanied by the appearance of heartburn. The pathogenesis of GERD is traditionally associated with a weakening of protective factors (normal barrier function of the lower esophageal sphincter, effective esophageal clearance, preserved resistance of the esophageal mucosa) and increased aggression factors (acid gastric and alkaline duodenal). With alcohol abuse, almost all of the indicated links in the pathogenesis of GERD occur. There is also a direct toxic effect of ethanol on the esophageal epithelium, which worsens its resistance and increases the risk of defects in the esophageal mucosa. Alcohol, regardless of the type of alcoholic drink, due to its stimulating properties, increases the acidity of the stomach and often worsens its evacuation properties, which leads to increased factors of aggression. Smoking and alcohol are factors that contribute to the development of esophagitis in patients with GERD initially without inflammation in the esophagus, and increases the risk of developing Barrett's esophagus (a precancerous change in the esophagus).
Back in the 60s of the last century, studies appeared indicating an increased risk of esophageal cancer with alcohol abuse. According to some authors, up to 50–75% of esophageal tumors are associated with alcohol consumption. Alcohol, when consumed daily, has been found to increase the risk of cancer of the mouth, pharynx, esophagus and larynx by 30%. Mortality from cancers of the mouth, pharynx, esophagus and larynx is strongly associated with levels of alcohol consumption over the previous 20 years. It has been established that smoking increases the risk of squamous cell carcinoma of the esophagus by 7 times, and with alcohol abuse - by 3 times. Alcohol increases the risk of developing both squamous cell carcinoma of the esophagus and adenocarcinoma of the esophagus, but more so of squamous cell carcinoma. Many studies have found that the risk of developing esophageal cancer increases with a combination of alcohol abuse and smoking, and, on the contrary, it decreases with an increase in the diet of vegetables and fruits. Thus, there is some synergy between the carcinogenic effects of alcohol and smoking. One of the likely explanations for the effect of alcohol on the development of esophageal cancer is the carcinogenic effect of acetaldehyde, a metabolite of ethanol. Ethanol begins to be metabolized into acetaldehyde already in the oral cavity under the influence of normal oral microflora, which leads to a significant increase in the content of acetaldehyde in saliva. A similar increase in the concentration of acetaldehyde in saliva is also observed during smoking. When swallowing, salivary acetaldehyde enters the pharynx, esophagus, and stomach, being a dose-dependent local carcinogen.
A rare but dangerous manifestation of the possible pathogenic effect of alcohol on the esophagus is the possibility of linear ruptures of the esophageal mucosa in the area of the esophagogastric junction (Mallory-Weiss syndrome), which is possible due to severe vomiting in response to alcohol intoxication, especially against the background of alcoholic esophagitis.
Alcohol abuse is also one of the causes of another rare (0.2–0.3% of esophagoscopies), but dangerous lesions of the esophagus - acute necrotizing esophagitis (acute esophageal necrosis). Endoscopic examination reveals black, necrotic mucosa of the esophagus, mainly in its distal parts (“black esophagus”). Acute necrotizing esophagitis is clinically manifested by bleeding in more than 70% of cases and can be complicated by stenosis or stricture, perforation, mediastinitis, and abscesses. The mortality rate for this pathology, according to researchers, is 31.8%.
And finally, we must not forget about another potentially dangerous manifestation of the effect of alcohol on the esophagus, which, however, is not a direct, but an indirect consequence of the pathogenic effect of alcohol - this is the appearance of varicose veins of the esophagus with portal hypertension due to alcoholic cirrhosis of the liver. In 50% of patients with alcoholic cirrhosis of the liver, esophageal varices develop within 2 years, in 70–80% - within 10 years from the date of diagnosis. Varicose veins are a potentially dangerous condition due to the risk of massive bleeding, which poses a threat to the patient's life. The risk of bleeding increases significantly with sharply dilated convoluted varicose veins of the third degree, with the presence of red marks on the surface of the varicose veins, with localization of varicose veins proximal to the zone 3–5 cm above the gastroesophageal junction, with severe cirrhosis in combination with the use of alcoholic beverages. After a successfully stopped episode of bleeding from esophageal varices, there remains a high risk of recurrent bleeding, especially in the first 6 months.
Treatment of various forms of alcoholic lesions of the esophagus depends on the nature of the lesion and involves an unconditional cessation of drinking alcoholic beverages. In the treatment of GERD, along with lifestyle modification, the drugs of choice are proton pump inhibitors, prokinetics, and antacids.
The main mechanism of action of proton pump inhibitors is to block the acid production of the stomach, thereby preventing the reflux of acid into the esophagus and limiting the contact of the esophageal epithelium with an aggressive acid factor. Among the proton pump inhibitors that have been used successfully for a long time, the drug pantoprazole should be noted. Pantoprazole has a sufficient antisecretory effect to reduce clinical symptoms and achieve endoscopic remission. It is actively prescribed for GERD and other acid-related diseases. The average dose of pantoprazole is 40 mg 2 times a day, the maintenance dose is 40 mg 1 time a day.
Another proton pump inhibitor, omeprazole, deserves attention due to its injectable form. Parenteral administration of omeprazole makes it possible to achieve in the shortest possible time the necessary increase in intragastric and intraesophageal pH, which is the most appropriate and necessary in urgent situations (for example, with ulcerative bleeding, perforated ulcers, acute pancreatitis and other similar conditions). Another justified use of parenteral forms is when the patient is unable to take a proton pump inhibitor orally on their own (for example, for the prevention of erosive and ulcerative lesions and possible bleeding in patients with critical conditions, with acute necrotizing esophagitis). The average dose of omeprazole for intravenous infusion is 40–80 mg.
Antacids have a rapid symptomatic acid-neutralizing effect in combination with an enveloping and adsorbing effect.
To correct motor disorders of the esophagus, especially with insufficient obturator function of the lower esophageal sphincter, prokinetics can be used - mainly dopamine receptor blockers (domperidone).
In the case of varicose veins of the esophagus due to liver cirrhosis of alcoholic or other etiology, the mandatory method of primary prevention of bleeding is the use (in the absence of contraindications) of a non-selective beta blocker - propranolol (anaprilin). There are also endoscopic methods for treating this pathology. An important direction of treatment is etiotropic therapy depending on the etiology of liver pathology. Often there is also a need to use hepatoprotective drugs of various types (ursodeoxycholic acid, essential phospholipids, amino acid-based drugs, herbal hepatoprotectors and others).
Thus, alcohol has a diverse effect on the esophagus, causing various pathologies. This once again confirms the long-known truth about the need to limit alcohol consumption in the population in order to prevent many diseases, including diseases of the esophagus.
Emergency measures
In such a situation, it is very important to take emergency care in time, this will help avoid complications:
- In case of a chemical burn to the throat, it is necessary to stop all contact with the aggressive substance.
- If a Lugol burn occurs on your throat, you should drink cold milk in small sips. This will cool the affected area and flush out the stomach at the same time.
- In order to relieve pain, you can use a solution of Novocaine or Lidocaine.
- To reduce swelling during a Lugol burn, take any antihistamine: Loratadine, Fenistil, Diazolin.
It is important to alleviate the condition of the victim; to do this, you need to provide a flow of fresh air and go outside. The patient must be silent, the muscle tissues and ligaments need rest!
Providing medical assistance to the victim
At the prehospital stage, emergency care is provided to the victim by ambulance staff. In this case, doctors carry out the following activities :
- The type of damaging agent is determined (from the victim himself or from surrounding people);
- Assessment of the general condition and examination of the throat mucosa;
- Analgesics for parenteral administration are used for pain relief. In severe cases, narcotic analgesics are used, when the risk of developing painful shock is high;
- Symptomatic therapy according to indications. When blood pressure increases due to stress, antihypertensive drugs are used, for heart pain, Nitroglycerin, and so on;
- In case of chemical burn injury, gastric tube lavage can be performed;
- Hospitalization of the patient to the hospital.
Hospitalization is required in the following cases:
- Any burns of the throat mucosa in children (in them this pathology is much more complicated than in adults);
- Deep burns;
- Violation of general well-being due to a burn (hypertensive crisis, cardiac arrhythmia, shortness of breath, and so on);
- Chemical burns in children and adults.
Description and causes of injury
A laryngeal burn is damage to the mucous membranes that occurs as a result of exposure to high temperatures or aggressive chemicals. This injury is quite widespread in everyday life, because a burn to the pharynx can be caused by consuming hot food and drinks. Damage from alcohol or acetic acid, Lugol, iodine, caustic alkalis, and concentrated steam is often found.
Experts consider a chemical burn to the throat to be the most difficult in terms of treatment and further recovery. Even a visit to the dentist can provoke injury, for example, if arsenic or other potent drugs come into contact with the mucous membranes of the larynx.
Young children are also susceptible to this type of damage and, due to their curiosity, may well try household chemicals. According to the international classification, burn injuries to the throat are divided by specialists into 3 degrees:
- Burn of the nasal mucosa: causes, symptoms, treatment methods
- The first degree is characterized by redness of the larynx and swelling of the mucous membranes.
- The second degree - manifests itself with specific blisters and the formation of gray films on a red and swollen throat.
- Third degree - manifested by necrosis of the affected tissues. Muscle tissue, ligaments and cartilage tissue are affected.
Lesions of the larynx of the second and third degrees require competent and timely assistance to the victim. Otherwise, extremely serious consequences are possible in the form of an attack of suffocation, poisoning, scarring and even the death of the patient!
Severity of burn injuries
Depending on the type of damaging factor, burns are classified as follows::
- Thermal burns of the throat mucosa. Aggressive agents in this case are steam, hot drinks or food;
- Chemical burns to the mucous membrane of the throat occur upon contact with various chemicals (acids, alkalis, alcohols).
Burns are divided into 3 groups according to severity:
- Mild (1 degree of severity). The top layer of cells is affected. In this case, there is the appearance of a slight pain in the throat when swallowing, a slight burning sensation and a change in the shade of the mucous membrane (it becomes white);
- Moderate severity (grade 2). Blisters appear on the surface of the mucous membrane, and after opening, ulcerations occur. The mucous membrane becomes gray;
- Severe (grade 3). Deep damage. The affected tissues die. Purulent wounds form. The general condition of the victim is severely impaired (intoxication). After a burn injury, massive scars remain that narrow the lumen of the throat.
Frequently asked questions to the doctor
ethnoscience
Good afternoon The daughter mistakenly took a sip of medical alcohol and mistook it for water. First there was vomiting. Then my daughter began to choke. I called an ambulance and she was taken to the hospital. They say she burned her neck. Please tell me how to quickly cure a burn of the larynx with alcohol? Maybe there are some traditional methods? They won’t let me leave the hospital, but we wanted to go to the seaside. Daughter is 10 years old.
Hello! Traditional medicine methods are ineffective in this case. I advise you to trust the doctors and complete the course of treatment.
Symptoms of a throat burn
Symptoms of burns are the same when the mucous membrane is exposed to both high temperatures and chemicals. The main symptoms of chemical and thermal burns of the throat mucosa are:
- Severe pain at the time of injury, which intensifies when swallowing;
- Intense burning , which in mild cases goes away after some time, but in severe cases it bothers you for quite a long time;
- Swallowing problems with more severe damage to the mucous membrane;
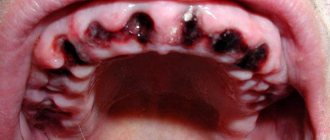
- The mucous membrane changes color . In case of a mild burn, it is hyperemic; in more severe cases, areas of white and gray color are noted. The photo shows what throat burns look like;
- Increased salivation;
- Voice change. He becomes hoarse. In some cases, the patient cannot speak;
- Inflammation of regional lymph nodes. They become painful on palpation, and their size increases;
- With severe burn wounds, breathing problems are observed in the form of severe shortness of breath and rapid heartbeat;
- A sharp disturbance in the general condition is associated with intoxication in severe burn injuries.
Main reasons
Burns of the laryngeal mucosa occur in both children and adults. Depending on the damaging factor, chemical and thermal burns are distinguished. The injury is rarely isolated and is usually combined with damage to the oral cavity, pharynx and esophagus.
Chemical damage to the mucosa
| Ethanol | A burn of the larynx with alcohol occurs: |
- with careless treatment of tonsils;
- ingestion of medical alcohol or tinctures (intentionally or by mistake).
Minor 1st and 2nd degree burns in adults do not pose a threat to life.
Treatment of a burn to the throat mucosa at home
Only minor burns are treated on an outpatient basis (that is, at home). In addition to the use of medications, it is necessary to observe a protective regime.
Food should be gentle (no hot and spicy seasonings, sour foods excluded, mashed, pureed), it should not be hot. For drinks, it is recommended to drink water and weak and not hot tea.
Use of drugs
Chemical and thermal burns of the throat can be treated at home using various groups of drugs:
- Antiseptics : Miramistin, Furacilin, Tantum Verde. These solutions are used to gargle and treat the mucous membrane. They destroy pathogenic flora;
- Painkillers (Analgin, Tempalgin, Baralgin) in the form of tablets and injection solutions. In the hospital, potent and narcotic drugs are used. This is necessary to eliminate pain;
- Antihistamines in the form of tablets and solutions for oral and parenteral administration (Suprastin, Loratadine, Diazolin). They are necessary to reduce swelling, itching and burning;
- Sedatives are prescribed to relieve stress and anxiety. Such drugs include tincture or tablets of valerian, motherwort, and so on;
- antibiotics are indicated in cases where there is a high risk of infection. Antibacterial drugs are prescribed only by the attending physician. Self-medication in this case is not acceptable.
Traditional methods
There are a large number of folk recipes that will help treat a burnt throat.
Folk remedies that will help in the treatment of chemical, thermal burns of the throat and burns after radiation therapy:
- For gargling, decoctions of herbs that have an anti-inflammatory effect are used. Such medicinal herbs are chamomile, yarrow and calendula. A decoction is prepared either from one plant or from a combination of herbs;
- If you burn (burn) your throat with hot food (food) or tea, the following dairy products will help: sour cream, milk, cream and butter. These foods should be kept cool. In this case, cooling and softening of the burn occurs;
- Treat the affected mucous membrane with sea buckthorn or olive oil;
- Rosehip decoction can be used for rinsing and ingestion. It has a general strengthening and anti-inflammatory effect.
Treatment
In case of a burn in the upper respiratory tract, after emergency care is provided, the victim is hospitalized in a hospital.
The extent of treatment depends on the cause of the burn and the severity of the injury.
Stages of therapy
| Call a medical team | Provide the operator with a detailed description of the situation. |
| Determine the cause of the burn | Interviewing witnesses to the incident and a careful examination can help with this.
|
| First aid | For a thermal burn:
In case of a chemical burn, it is recommended:
|
Prednisolone
After their condition improves, patients are transferred to the burn department. If it is necessary to continue intensive care, go to a specialized intensive care unit.
Nebulizer therapy for laryngeal burns
Positive results of inhalation therapy on the second day after injury:
- reducing swelling of the mucous membrane of the upper respiratory tract;
- elimination of respiratory failure;
- reduction of inflammation;
- restoration of swallowing;
- elimination of aphonia.
The recommended duration of the procedure is 10 minutes. Inhalations are carried out twice a day.
Aerosol mixture recipe:
- 50 ml 0.9% sodium chloride;
- "Trypsin" -10 mg;
- 2.5% hydrocortisone solution – 5 ml;
- 2.4% aminophylline solution – 1 ml;
- 4% sodium bicarbonate solution – 4 ml.
Also, good results are provided by inhalation of sympathomimetics (adrenaline), drugs that dilute sputum (acetylcysteine). The duration of the course is 7 days.
After reading the article, you will learn everything about how to treat a burn of the larynx and throat.