Swallowing is a complex set of motor reactions that move food from the mouth through the esophagus to the stomach. The swallowing reflex is innate. It is important to note that during the correct act of swallowing, the tip of the tongue should normally rest against the anterior third of the hard palate.
A child is born with a well-developed swallowing mechanism, which in the first months is called infantile . Due to the contraction of the muscles of the lips, cheeks, and tongue during sucking, negative pressure is created in the baby’s mouth and milk enters the mouth, and the tongue, located between the toothless gums, directs the milk into the oropharynx. Before the first teeth erupt, this infantile type of swallowing , in which the tongue rests on the lips, is a physiological norm . But as baby teeth erupt, sucking is replaced by chewing, and the child’s type of swallowing changes to somatic . During somatic swallowing, the tongue is located in the anterior third of the hard palate, while the back of the tongue pushes food into the larynx.
If a child constantly consumes liquid or semi-liquid food, despite the presence of teeth, then a full act of chewing is not formed, and the transition from the infantile type of swallowing to the somatic one does not occur. At the moment of swallowing, a child with an infantile type of swallowing places his tongue between the upper and lower rows of teeth, which contributes to the formation of an open bite. In this case, the perioral muscles are involved in the act of swallowing, i.e. the lower part of the orbicularis oris muscle, the mentalis muscle and the neck muscles noticeably tense, which is easy to detect by asking the child to swallow saliva.
An incorrect type of swallowing can also result from:
- Using a long pacifier that occupies the entire mouth of the infant and touches the soft palate, which interferes with the proper function of the tongue, soft palate and pharynx.
— Disturbances also occur when there is a large hole in the nipple, through which milk and milk formulas enter the oral cavity in large quantities, the child choke on the incoming food and can swallow it only after the nipple is removed from the mouth and the food flows out through the corners of the mouth. In this case, the forward position of the tongue, which regulates the flow of milk, can become fixed and cause improper swallowing.
— Chronic tonsillitis and adenoid growths also contribute to the tongue moving forward.
- If a child constantly consumes liquid or semi-liquid food, despite the presence of teeth, then a full-fledged act of chewing is not formed, and the transition from the infantile type of swallowing to the somatic one does not occur.
With the infantile type of swallowing, the child’s tongue gets used to only the simplest movements, so the lingual muscle develops poorly (the tongue is not sufficiently developed and mobile).
Infantile breathing
Swallowing is a certain set of motor reactions that ensure the normal passage of food from the mouth to the stomach through the esophagus.
During the correct act of swallowing, the tip of the tongue rests on the anterior third of the hard palate. Many people believe that swallowing is a reflex reaction of the body, i.e. to the same as salivation, breathing, reflexive withdrawal of the hand in case of touching something hot, etc. In other words, they believe that swallowing is wrong - it is impossible. But, unfortunately, this phenomenon is not so rare and is called infantile swallowing.
Common symptoms of dysphagia
At the initial stage of the pathology, patients complain of problems when swallowing solid food, which are accompanied by discomfort in the larynx. The characteristic symptoms of this disorder are as follows:
- excessive salivation (or inability to swallow saliva);
- hoarseness or hoarseness of voice;
- dry cough;
- feeling of lack of air and distension behind the sternum;
- sore throat.
As the pathology progresses, a person has problems swallowing liquids. There is anxiety about eating, food getting into the respiratory organs. If no correction methods are taken, the person’s general condition of the body worsens, and body weight also decreases significantly.
Bite problems begin in early childhood
The health of first the child and then the adult depends on the attention and care of parents.
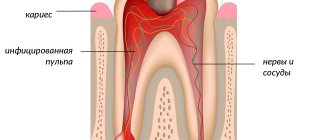
But often parents do not pay attention to how the first teeth grow; anyway, they will fall out and there will be new ones. They believe that it is normal not to treat even caries and pulpitis, let alone crooked teeth, their uneven location in the jaw, a frenulum that is too large or, conversely, too small. It seems to them that all children suck their thumbs or constantly breathe through their mouths. Parents do not see such “little things” as a problem. They think that it is too early, and after replacing the teeth with permanent ones, everything will return to normal on its own. So why waste money and torture a child? Unfortunately, with the formation of a permanent bite, all milk problems do not go away, but, on the contrary, begin to actively worsen. A person enters adult life with an ugly smile, an incorrect bite and, often, with deformation of facial proportions. And this is only the visible part of the troubles; problems with bite affect the entire human body. Read more about this in our article on adult orthodontics.
On this page you will learn everything parents need to know so that their child has a healthy bite and straight teeth.
Symptoms of infantile swallowing
With infantile swallowing, the following signs are present:
- The lips are closed or open, but when swallowing food they are compressed even more tightly due to contraction of the muscles of the mouth.
- The tongue rests on the lower teeth, or is located between the upper and lower rows of teeth.
- The muscles of the neck and the mental muscle are also involved in the implementation of infantile swallowing.
With this condition, the lower part of the face turns out to be very tense, which can be seen in pinpoint pits in the corners of the mouth and on the skin of the chin. Due to the fact that the neck muscles are involved in the swallowing process, it involuntarily stretches.
Diagnostics
In most cases, infantile swallowing leads to malocclusion. Problems with swallowing are most often identified during additional examination:
- Examination by a dentist. The specialist detects defects in the dentition and mouth breathing. The easiest way to detect it is to swallow water in small portions.
- X-ray of the pharynx and esophagus, which helps to trace the movements of the tongue, as well as estimate the time of swallowing.
- Examination of the nasopharynx. A specialist performs pharyngoscopy and nasal endoscopy.
- Speech therapy diagnostics. A speech pathologist evaluates the relationship between infantile swallowing and incorrect pronunciation of sounds. During the examination of oral speech, lateral, interdental pronunciation and other defects are revealed.
Diagnostics
After the patient is admitted to the department, the quality of swallowing is assessed using a special dysphagia rating scale.
According to the severity of this pathology, 4 degrees are distinguished. With the first, there are problems with swallowing solid foods, with the second, a person can only swallow liquid food. In the third degree, there is difficulty swallowing both solid and liquid food, and in the fourth degree, a person cannot even swallow his own saliva.
When collecting anamnesis, it is necessary to clarify:
- What kind of food intake causes problems with swallowing (problems with swallowing solid foods are more typical for the esophageal form of the pathology, liquid - for the oropharyngeal).
- The time interval between the act of swallowing and the feeling of a “coma”. The feeling of a “coma” in most cases excludes a mechanical cause for this condition.
- The nature of the increase in symptoms. If the nature is progressive and short (less than three months), then a malignant tumor can be suspected.
- The presence of heartburn, regurgitation, coughing while drinking and eating.
Why does a child need an orthodontist after early milk tooth extraction?
Has your child had a baby tooth removed, but the permanent one is still a year or more away? Then there is a danger that the baby’s bite will deteriorate. After removal, neighboring teeth will really want to move and take up the vacated space. If you do not install a special prosthesis or a special orthodontic spacer, then the permanent tooth will have nowhere to go, and it will erupt where necessary, and not where it should. In this case, it is impossible to do without the intervention of an orthodontist.
Therefore, dear fathers and mothers, let’s agree that if a child under 5 years old has gaps in his teeth, then at a minimum he definitely needs a consultation with an orthodontist!
Treatment of dysphagia
How dysphagia will be corrected depends on the type of disorder:
- Drug treatment. Medicines are prescribed that reduce the acidity of gastric juice, and antibiotics may also be prescribed. Use of all medications only under the supervision of a physician.
- Surgical intervention. Surgery is prescribed if there is no effect from medications and other treatment methods. Most often, surgery is necessary in the case of burns, cancerous tumors and severe inflammatory lesions.
- Diet therapy. Fatty, fried, smoked, spicy and spicy foods, including fast food, are excluded. Food should be chewed thoroughly to avoid large chunks of food being swallowed. Eat small, frequent meals.
- Speech therapist classes for dysphagia. The recovery process of speech disorders is carried out in conjunction with the treatment of the underlying disease that caused the disorder.
What is dysphagia
Dysphagia is a violation of the complex reflex swallowing act. The ICD-10 code is R13. This is a secondary pathological process that develops against the background of other diseases. This condition is manifested by the inability or difficulty of swallowing, pain when swallowing, liquid or food getting into the trachea, larynx and nose.
Dysphagia must be distinguished from odynophagia, which is defined as a sensation of pain when food passes through the esophagus. This condition must also be distinguished from the sensation of a lump in the throat, when a person feels that something is stuck in the back of the throat. In this case, dysphagia is a symptom that appears only when attempting to swallow.
Classification and symptoms
Pathology varies depending on the location of the lesions, causes and severity.
| By place of education | |
| Oropharyngeal (oropharyngeal) | The location of the lesion is the oropharynx area . The food lump moves from the pharynx into the esophagus with difficulty. During swallowing, the child begins to choke, causing food to enter the trachea or nasal cavity. Oropharyngeal dysphagia occurs as a result of disruption of the neuromuscular connection. Characterized by a severe cough and increased salivation. In order for food to pass through the esophagus, the baby has to make efforts. |
| Esophageal | The lesion occurs in the lower region of the esophagus, and difficulty swallowing appears in the cervical region. The symptoms of esophageal dysphagia are similar to oropharyngeal dysphagia, so a doctor can make an accurate diagnosis during an examination. Characterized by frequent belching with a sour taste, severe heartburn, and pain in the chest cavity. |
| Cricopharyngeal | A disorder in the contraction of certain fibers, which causes relaxation of the cricopharyngeal muscle. This contributes to bulging of the walls of the esophagus and the formation of lung pathologies. |
| By appearance | |
| Paradoxical | The child has difficulty swallowing, but solid food passes better than liquid food. Often occurs against the background of diseases of the esophagus. If tumors are present, the baby may begin to refuse solid foods, then semi-liquid foods and drinks. There are cases when dysphagia disappears. But this is an imaginary remission and the disorder will soon make itself felt. |
| Neurogenic | The nervous system is affected. The formation of a food bolus in the oral cavity is difficult or the bolus simply does not pass through the esophagus. Neurogenic dysphagia can be caused by severe traumatic brain injury or stroke. |
| Sideropenic | Dystrophic changes in the mucous membranes of the esophagus. This may be indicated by a deficiency of iron and nutrients in the body, which leads to pathological changes in the swallowing muscles. It can be either a genetic or acquired disorder. |
| Psychogenic | Occurs due to frequent stress and nervous tension. While eating, the baby feels a “lump” in the throat and pain in the chest area. Severe heartburn may occur. |
| Due to the occurrence | |
| Functional (nervous) | A disorder of the esophagus resulting from a disorder of the nervous system. The child has difficulty swallowing food, may refuse to eat, gag reflexes, and breathing and sleep disturbances occur. |
| Organic | As a result of diseases that led to disorders of the oropharynx and esophagus. |
Main reasons
Problems with the passage of food through the pharynx and proximal esophagus are caused by the following reasons:
- Mechanical obstruction. It can be caused by inflammatory processes, enlarged lymph nodes, thyroid hyperplasia, muscle fibrosis, etc. Narrowing of the upper digestive tract can also be a consequence of malignant tumors of the pharynx, oral cavity and larynx.
- Quincke's edema and foreign body obstruction are often a consequence of acute esophageal dysphagia.
- Narrowing of the lumen of the esophagus. This happens with stomach cancer, malignant tumors in the esophagus, and eozonophilic pharyngitis. Signs of pathology are observed when the lumen of the esophagus narrows to less than 12 mm.
- External compression of the esophagus. These can be chest tumors, enlarged midwall lymph nodes, as well as various infectious diseases - histoplasma, tuberculosis, etc.
- Impaired coordinated contraction of the esophageal muscles. Occurs in diabetes mellitus, scleroderma, achalasia. The contraction of the esophageal muscles, which prevents swallowing, is affected by the intake of estrogens, nitrates, and calcium channel blockers.
Why does an orthodontist often work together with an ENT doctor?
Breathing problems rank third among the causes of improper development of the dental system in children, after genetic and hereditary ones.
It is important to understand why a child’s bite is deteriorating and not to miss the moment. A good orthodontist will check whether the child is breathing correctly, and if mouth breathing is suspected, he will immediately involve an ENT specialist.
As we wrote above, correcting a malocclusion is possible only after the child learns to breathe through his nose again. To do this, you need to cure diseases that interfere with nasal breathing. Most often you have to deal with inflammation of the nasal and nasopharyngeal mucosa, sinusitis and proliferation of adenoid tissue. This is what an ENT doctor does.
Exercises to correct infantile swallowing
In order for a child to learn to swallow correctly, a certain set of exercises is carried out:
- Mouth in a half-open position. We lick the lower and upper lips, running the tongue from one corner of the mouth to the other.
- Painter. We smile and open our mouths. With the wide tip of the tongue we stroke the palate from the teeth to the throat. Make sure that the lower jaw remains motionless during the process.
- Swing. We try to reach the chin and nasal septum with our tongue.
- We brush the upper teeth. We smile and open our mouths. Using the tip of the tongue, we clean the upper incisors from the inside, moving them from side to side.
- We count the upper teeth. We smile and open our mouths. With the tip of the tongue we rest in turn on each tooth of the upper row from the inside. The lower jaw should remain motionless.
- Horse. We smile and open our mouths. Click your tongue, imitating the sound of a horse's hooves. The mouth is in an open position, the tip of the tongue is not pointed or extended. It is important that the tongue does not tuck inward and the lower jaw does not move. Number of repetitions – 50-60 times.
- Football. The mouth is closed, the tip of the tongue is alternately pressed against the cheeks so that the balls “inflate” under them.
- Use an exercise with a spatula, a tube, a pencil - position it so that the spatula (pencil, tube) is across the dentition, and hold it with clenched teeth. The tip of the tongue is moved either above or below the spatula, tube, or pencil.
- Learning to swallow.
- Place a rubber ring on the tip of your tongue (you can cut it from a regular pipette). The child raises his tongue upward and presses it to the anterior part of the hard palate in the area of the palatine folds, clenches his teeth, and closes his lips (initial position). You need to ask him to swallow saliva without changing the position of the tip of his tongue and the rubber ring. If the tongue is between the teeth, then the exercise is performed incorrectly. It is necessary to tactfully explain to the child the purpose of this exercise. The exercise is repeated on the first day 5-6 times, on the second - 2 times (morning and evening) 5-6 times. In the following days - 3 times a day, 10-12 times.
- The starting position is the same. Only now your child must hold the ring in this position for 5 minutes. On subsequent days, the exercise time is increased to 10 minutes.
- The starting position is the same. Now you will teach your child to swallow correctly, without lifting his tongue from the palate, ask him to swallow saliva with his lips closed. The exercise is repeated 3 times a day, 10 times. In this case, you need to ensure that your lips are relaxed.