The branch of dentistry such as orthodontics continues to develop. Today, there are many different orthodontic treatment methods that help not only improve the aesthetic appearance of the smile, but also normalize the function of the jaws.
Medicine does not stand still; orthodontics is developing more and more every year. Patients become more knowledgeable about smiles and attractiveness. More and more patients are complaining about a narrow smile; they want others to see as many teeth as possible when smiling. How and due to what, and most importantly at what age and what can an orthodontist do? Expansion of the upper jaw can be divided into conservative and surgical. It can also be divided into treatment in childhood, in mixed dentition and in adulthood when all teeth are permanent
Expansion of the upper jaw is indicated in the following cases:
- Micrognathia is underdevelopment of the upper jaw. It may be a consequence of rickets, endocrine diseases, injuries, too early loss of milk or permanent teeth, etc.
- Narrowing of the dentition of the upper jaw , resulting in a pathological crossbite.
- Difficulty in nasal breathing due to insufficient volume of the nasal cavities.
- Mesial occlusion.
- Protrusion of incisors.
Next, we will tell you what methods of expanding the upper jaw exist, what types of non-removable devices there are and what a non-removable plate for expanding the upper jaw is, as well as how the expansion is carried out surgically (surgery).
Horizontal jaw distraction followed by orthognathic surgery
R. A. Khachatryan , Ph.D., maxillofacial surgeon, implantologist, scientific advisor to Biotech International (France) and Medtronic (Russia), consultant to the dental clinics “Kolibri” (Krasnodar), “Visit” (Anapa) )
Micrognathia of the jaws is one of the common pathologies among patients with disharmony of the facial skeleton. It is expressed in transversal underdevelopment of the jaw bones in combination with the inevitable crowding of the dentition, malocclusion, reduced volume of the oral cavity, and impaired chewing and speech functions. A separate contingent consists of patients with obstructive sleep apnea.
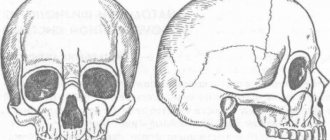
Often transversal disharmony of the dentition is combined with skeletal abnormalities of the jaws (Fig. 1, 2).
Rice. 1. A patient with a combined pathology of the facial skull - retromicrogenia of the upper jaw in combination with progenia of the lower jaw, class III occlusion.
Rice. 2. A patient with a combined pathology of the facial skull - retromicrogenia of the upper jaw in combination with progenia of the lower jaw, class III occlusion.
The aesthetic proportions of the face in this pathology are disturbed, which often leads to severe disturbances in the psycho-emotional status of patients.
Well-known methods of treating this pathology, consisting of bilateral removal of premolars with subsequent orthodontic correction of the dentition, do not lead to a complete restoration of the reduced transversal volumes of the jaws and oral cavity, as well as the corresponding functional parameters of the dentoalveolar system.
Orthopedic methods for correcting transversal deficiency of the body of the upper jaw were first described in 1860, and were subsequently modified and improved many times. The goal was to quickly expand the upper jaw by activating an intraoral distractor fixed with half rings and bars in the area of the dentition. The expansion rate was 0.5 mm per day.
Such orthopedic expansion of the upper jaw using fixed orthodontic appliances has many disadvantages and complications. In the world literature and according to our observations, undesirable secondary effects of orthopedic expansion are noted, expressed in the resorption of the cortical plates of the jaws and tooth roots, gum recession with the occurrence of periodontal pathology and frequent relapses of deformities. The method also has limited age indications and is used at a young age during the period of active growth of the bones of the facial skull up to 14 years in girls and up to 17 in boys.
Rapid expansion of the jaws using a previously performed osteotomy is the technique of choice in patients with complete growth of the facial bones, as it eliminates any bone resistance during lateral movement of osteotomized jaw fragments. This type of surgery is based on stretching a blood clot retracted between osteotomized fragments with its subsequent mineralization and ossification; it is known in the literature as the phenomenon of distraction osteogenesis (Fig. 3-5).
Rice. 3. Crowding of the upper jaw dentition, micrognathia.
Rice. 4. The transpalatal distractor installed intraoperatively is the end of the distraction period.
Rice. 5. Final orthodontic correction of occlusion.
This paper presents methods for surgical osteotomy of the jaws followed by the use of the distraction method using fixed orthodontic structures or jaw distractors. Distraction devices are installed the day before surgery or intraoperatively, depending on the planned design.
On the upper jaw, the orthodontic distractor is fixed to the dentition using half-rings and rods (Fig. 6).
Rice. 6. Standard maxillary distractor fixed in the dentition area.
If there are problems with the dentition or partial secondary edentia of the upper jaw, intraoral distractors are used, which are installed intraoperatively (Fig. 4).
Surgery is performed mainly under general anesthesia - nasotracheal intubation with mechanical ventilation. After infiltration in the area of the vestibule of the oral cavity, an incision is made along the interdental gingival papillae. Incisions in the vestibule of the oral cavity are practically excluded from European protocols for orthognathic surgery.
After careful detachment of the mucoperiosteal flaps, the body of the upper jaw is exposed. Osteotomy of the maxilla represents a classic cut along the Le-Fort I line in combination with osteotomy of the nasal septum, lateral walls of the maxillary sinuses and pterygomaxillary areas (Fig. 7).
Rice. 7. Stage of horizontal osteotomy of the upper jaw.
Then the area of the median palatal suture is dissected (Fig. 8).
Rice. 8. Dissection of the median palatal suture.
After controlling adequate mobility of the osteotomized jaw fragments, the flaps are sutured.
In the area of the lower jaw, the distractor is fixed in the area of the dentition with the screw positioned vestibular or lingual. An incision in the frontal region is made along the interdental papillae in combination with lateral incisions in the canine area (Fig. 9).
Rice. 9. An incision in the frontal region along the papillae of the teeth.
After detachment of the mucoperiosteal flap, a linear cut is made in the area of the symphysis along the midline or a stepped osteotomy in front of the canines extending to the midline (Fig. 10).
Rice. 10. Median symphyseal osteotomy.
After complete mobilization of the fragments, the wounds are sutured tightly. The hospitalization period is 24 hours.
Postoperative management of the patient includes taking non-steroidal anti-inflammatory drugs, nasal vasoconstrictors and antiseptic mouth rinse. Activation of distractors begins on the 8th day of the postoperative period by the patient himself or a person from his close circle. The degree of screw activation depends on the required size of correction.
After completion of distraction to the planned width, a retention period of up to 6 weeks promotes ossification of the distraction zone and consolidation of jaw fragments.
Postoperative orthodontic treatment completes the morphological formation of the dentition. In the long-term postoperative period, if necessary, some patients with skeletal anomalies also undergo orthognathic surgery.
Clinical case of combined pathology of dentition, occlusion and facial bones
The patient, 26 years old, suffers from severe dentofacial dysmorphosis, expressed in micrognathia, crowding of teeth, retrogenia and long face syndrome (Fig. 11, 12).
Rice. 11. Occlusion of the patient before treatment.
Rice. 12. Occlusion of the patient before treatment.
At the first stage of treatment, after installation of an intraoral expander, surgical compactosteotomy of the upper and lower jaws is performed. Spontaneous closure of the diastema is noted even before the start of orthodontic treatment (Fig. 13-16).
Rice. 13. Patient 8 days after the start of distractor activation.
Rice. 14. Patient 8 days after the start of distractor activation.
Rice. 15. Patient 3 months after distraction—end of retention period.
Rice. 16. Patient 3 months after distraction—end of retention period.
The orthodontist fixes bracket systems on the dentition in order to prepare the occlusion for the second stage of surgical correction - orthognathic surgery.
Clinical examination of the patient before orthognathic surgery reveals a combined pathology of the skull - horizontal hypertrophy of the upper jaw in combination with microgeneia. The central incisors protrude excessively from under the upper lip, the mouth is open, the lips do not close. The posterior position of the lower jaw is also noted, the labio-mental fold is smoothed, and the tissues of the perioral area are tense.
The patient underwent a combination of horizontal osteotomy of the upper jaw for elevation and rotation, bilateral osteotomy of the branches of the lower jaw and aesthetic genioplasty (Fig. 17, 18).
Rice. 17. Occlusion of the patient at the end of the distraction period before orthognathic surgery.
Rice. 18. Occlusion of a patient after orthognathic surgery.
Thus, the method of surgical-orthodontic expansion of the jaws eliminates the resistance of the jaw bones to the lateral movement of osteotomized fragments, sharply reduces the time of treatment and rehabilitation of patients, and minimizes the number of recurrences of deformities.
In the operated group of patients, there was a complete restoration of the function of chewing and speech, harmonization of facial features and, as a result, a significant improvement in the emotional state of the patients.
Conservative treatment methods, or a fixed device for expanding the upper jaw
In children, the most effective way to expand the upper jaw at the moment is a plate with a screw in the structure. The plates are removable and non-removable. All scientific studies show that an orthodontic structure works most effectively only if it is in the mouth for at least 24 hours a day, hence the conclusion that a non-removable technique works much more effectively than a plate that a child can remove at school, rest, lose, and so on. .
HAAS device
The most common and convenient to use for both parents and doctors is the non-removable HAAS device. The device is fixed to the temporary teeth on the upper jaw by an orthodontist; it is absolutely invisible to others, but clearly and quickly performs its task. The most successful and appropriate time to work on it is when the central incisors are replaced with permanent ones, i.e. at the age of 7-8 years. The expansion of the upper jaw is carried out through the work of a screw, which the parents themselves tighten based on the recommendations of the attending physician.
Complex orthodontic treatment
Stage I
The first point of the treatment plan was performed by maxillofacial surgeon I.I. Yakimenko. The operation took place in a hospital setting under anesthesia. Before the operation, professional dental hygiene was performed - removal of plaque and tartar (hygienist Sorokina D.).
The intervention is performed through the oral cavity, so no scars are left on the face. A special distraction device is installed in the palate area. After the operation, the patient remains in the hospital for about 10 days, the surgeon monitors the healing process. On days 6-7, the attending physician performs the first activation of the device. Further activation of the device is also performed by the surgeon, gradually, as much as necessary (in millimeters), until the required width of the dentition is achieved.
The photo shows a view with the distraction device installed before fixing the braces:
Stage II
Orthodontist M.P. Sleptsova installed reliable Victory metal ligature braces on the lower jaw and aesthetic, inconspicuous Clarity ceramic braces on the upper teeth. After activation, wearing the palatal distraction device continues for another 4 months. Before installing braces, all Dial-Dent patients receive professional teeth cleaning as a gift (hygienist Smirnova E.).
Removal of the device is performed under local anesthesia. Treatment with braces continues.
Photo after removal of the palatal apparatus:
Stage III
Double-jaw surgery to place both jaws in the correct position was performed by surgeon I.I. Yakimenko. In addition to the attending surgeon, a team of doctors takes part in the operation. The intervention is performed intraorally, leaving no scars on the face. The operation is performed under general anesthesia. Braces are not removed during surgery.
Healing lasted 2 weeks. Further treatment with braces was continued.
Stage IV
The final stage of teeth straightening using a brace system, wearing orthodontic elastics. This stage is very important and necessary to stabilize the results of treatment. At the stage of orthodontic treatment, professional teeth cleaning with braces is carried out to prevent the development of caries.
Retention
After removing braces, treatment does not end - a retention period begins. The orthodontist installed a non-removable wire retainer on the lower teeth, and a retention guard was made for the upper jaw, which must be worn while sleeping.
The recommended schedule for visiting the orthodontist during the retention period is once every 3 months.
Surgical expansion of the upper jaw
The surgical method for correcting the width of the upper dentition is that for an older patient and with the most pronounced defect of the upper jaw, the surgeon installs an apparatus in the area of the palatal suture, which carries out the “growth and expansion” of the jaw. Surgical expansion of the maxilla is the most effective method of expansion, although it is somewhat traumatic.
The device installed during the operation can be activated only on the third day. The first activation is carried out by the attending physician, and later this procedure can be carried out by the patient himself at home. The installed palatal expander must be worn for approximately 3-4 months after the maxillary expansion surgery has been performed.
In any case, the choice of method and determination of the period depends on the clinical picture, the desire of the patient and the capabilities of our dentofacial system.
Correction of any bite problems in children by our pediatric orthodontists:
- treatment with a smile, no stress for the child, no discomfort
- accurate diagnosis of more than 50 parameters before bite treatment
- treatment using both removable and non-removable equipment
- 100% solution to the problem of maxillary expansion
- noticeable treatment results after 2.5 months.
Expansion of the lower jaw
A narrow lower jaw, or microgenia, can be corrected in childhood with special devices - distractors. This is a device that gradually stretches the bones of the lower jaw. New bone and soft tissue grows at the site of the sprain. When installing a distractor, first increase the distance between the canines of the lower jaw. Every day the device allows you to increase the lower jaw by 1 mm. When the jaw is wide enough to accommodate tooth growth, the distractor is placed in place for at least two weeks to stabilize the sprain.
If you have a problem similar to that described in this article, be sure to contact our specialists. Don't diagnose yourself!
Why you should call us now:
- We will answer all your questions in 3 minutes
- Free consultation
- The average work experience of doctors is 12 years
- Convenient location of clinics
Single contact phone number: +7
Make an appointment
In adult patients, the lower jaw bones are fused and cannot be stretched, as in children. Therefore, to enlarge the lower jaw, the surgeon cuts the bone in several places with an ultrasonic knife. On the fourth day after surgery, an expansion device is installed. The first adjustment of the stretching is carried out by an orthodontist, then the patient himself controls the stretching process, which can take up to six months.
After expanding the lower jaw, braces are installed on the lower front teeth to correct the bite. Crowded teeth gradually occupy the resulting space.
The photo below shows a narrow jaw before and after expansion.