Indications
Indications for removal of the submandibular salivary gland are:
- chronic sialadenitis (inflammation);
- benign or malignant tumors;
- multiple cystosis;
- salivary stone disease;
- severe injury to the gland;
- complete blockage of the salivary ducts with the impossibility of restoring their patency.
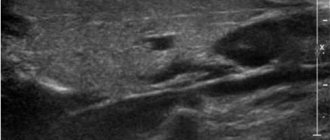
Depending on the diagnosis, various tests are prescribed before the operation - ultrasound, computed tomography or magnetic resonance imaging, chest x-ray. In the case of a tumor, a biopsy is also necessary to determine the nature of the formation. Salivary stone disease is examined using contrast sialography.
Indications for removal
The main reason for prescribing surgical intervention is the ineffectiveness of conservative therapy.
This often occurs with the development of the following diseases:
- Inflammatory process or sialadenitis. Develops against the background of exposure to a bacterial or viral infection. Symptoms are an increase in the size of the affected area, pain, a decrease in the volume of salivary fluid production, and general malaise.
- Pathological narrowing (expansion) of the excretory duct or sialodochitis. Symptoms are increased production of salivary fluid, a salty taste in the mouth, swelling, distension in the area, pain during eating, stuffy ears.
- Formation of stone-like deposits in the lumen of the gland or sialolithiasis. Surgical intervention is prescribed when the stone reaches a size of 1 mm, which clogs the duct and cannot be washed out by conservative methods. Symptoms are bloating, swelling, unpleasant taste in the mouth, periodic acute pain, difficulty swallowing saliva. At an advanced stage, general intoxication occurs.
- Bilateral swelling of a non-inflammatory and non-tumor nature or sialosis. Symptoms: local pain syndrome, impaired activity of the facial nerve.
- Mumps or mumps. Develops when the body is infected. Symptoms are swelling of the endocrine glands, high fever, loss or decreased appetite, general malaise, headache.
- Purulent lesion.
- The presence of a tumor-like neoplasm.
- Severe mechanical damage.
For sialodochitis and sialosis, surgical treatment is prescribed in extreme cases, if the swelling has reached its maximum size, thereby causing facial asymmetry.
Preparation for the operation and features of its implementation
Preoperative preparation includes:
- laboratory tests;
- abolition of blood-thinning medications (at least a week before the procedure);
- changing your diet three days before surgery - excluding alcohol, spicy and rough foods, hot drinks.
- Smoking is also prohibited before surgery.
Removal of the submandibular salivary gland is a complex and specific operation, since its anatomical location near the nerve and choroid plexuses, muscles and other organs is associated with risks of serious complications. Such a procedure can only be performed by experienced specialists - dental surgeons or maxillofacial surgeons.
In the case of a malignant tumor, especially when it grows beyond the gland, the organ is removed along with the affected tissue of nearby muscles and lymph nodes. In other cases, only gland tissue is removed.
Surgery to remove the submandibular salivary gland can be performed in several ways:
- The traditional method is surgical excision of tissue with removal of the pathological gland. This type of operation does not require specific equipment, which explains its lower cost and speed of implementation. Postoperative wounds are quite large; the time for suture removal varies from 1 to 3 weeks.
- A microsurgical endoscopic operation that does not require large tissue intersections - all actions are carried out using manipulators, and observation is carried out using a probe that transmits an image to the screen. The great advantage of this type of operation is the targeted effect, due to which in case of salivary stone disease, benign tumors and cystosis of the gland, there is no need for its complete removal - only a small area of it is excised. After the operation, small marks remain, the stitches are removed after a few days. The disadvantage of this method is its high cost.
Diagnosis of salivary gland cancer in Israel
The quality of the subsequent course of treatment depends on the accuracy of the diagnosis. Therefore, Israeli clinics use advanced equipment and modern techniques for examining patients. The following diagnostic methods are usually used:
- Examination and consultation with an oncologist.
- Ultrasonography. Ultrasound helps determine the location and size of the affected area of the salivary gland.
- MRI. During the session, the person lies motionless in the apparatus. All metal objects must be removed before the examination. Patients whose body weight is more than 150 kg are not required to undergo MRI. The duration of the examination is no more than an hour.
- Biopsy. Cells are collected from the tumor-affected area of the gland using a thin needle and syringe.
- CT scan. The procedure allows you to obtain an image of any necessary area of the patient’s body. If necessary, a certain amount of dye is injected into the vein. This is necessary to improve the quality of the pictures. The examination of one area lasts about 20 minutes. The dye is eliminated from the patient’s body on its own within a few days.
If the diagnosis has confirmed that the tumor is not malignant, its treatment is still recommended. The fact is that about eighty percent of benign tumors eventually degenerate into malignant ones. Cancer treatment in Israel is a priority. Specialists of the Tlv.Hospital consultation center will take care of all issues related to organizing the diagnosis and treatment of salivary gland cancer in Israel.
Performing surgery to remove the salivary gland
With the traditional method of surgery, the patient assumes a lying position with his head thrown back and to the side. The operation involves local infiltration anesthesia. Several parallel incisions are made in the submandibular area, the tissue is lifted, and the capsule of the salivary gland is discovered, which is opened, and the gland tissue is extremely carefully removed and removed. When a malignant tumor grows together with nearby tissues, the latter are also removed. After this, stitches are applied.
During endoscopic surgery, both local and general anesthesia can be used. Through small punctures in the tissue, manipulators and a video probe are inserted, which projects all the actions performed on the screen. When the manipulators reach the gland, small incisions are made with their help, through which pathological tissue is removed. The endoscopes are then removed and sutures are placed at the puncture sites.
Postoperative care of the surgical site includes:
- hygiene - no water or dirt should get into the wounds;
- special diet - the diet will consist of semi-liquid warm food, no hot or cold drinks, no alcohol;
- smoking ban;
- special treatment - it is recommended to regularly treat the seams with antiseptics, and the oral cavity after each meal should be rinsed with a mixture of antiseptic and water.
If all the recommendations of the attending physician are followed, complete wound healing occurs within a few months.
Removing a stone from the duct of the sublingual salivary gland
Clinical example : Removal of a stone from the duct of the sublingual salivary gland.
A 26-year-old female patient is bothered by a periodically swollen movable ball under her tongue. Does not hurt. I first discovered it, as she says, “from school,” i.e. about 8 years ago.
The salivary glands, as we know from the anatomy textbook, are divided into large and small - paired parotid, paired submandibular and sublingual. And many small salivary glands covering the main part of the oral cavity - cheeks, lips, area under the tongue. The epithelium lining the inside of the duct of each gland secretes a secret - the well-known saliva. And when the duct is blocked after trauma or a stone (this is salivary stone disease ), the secretion of saliva becomes difficult, so that it accumulates in the duct, which also continues to secrete saliva. In this area, the inner part of the duct walls gradually changes, the composition of cells changes and a cystic membrane is formed. Gradually, mineralization of the stone that blocked the duct occurs - and it, together with the cyst, gradually increases in size. In this case, 8 years have passed since the discovery, and the removed stone was almost 2 cm in length and 0.6-0.8 cm in width.
** – photo is not for the faint of heart (click to open):
The removed stone was almost 2 cm in length and 0.6-0.8 cm in width
Let's follow the entire course of the operation.
It practically does not protrude above the mucous membrane, only 3-5 mm; when pressing with fingers, the dense structure can be felt quite easily. This formation is mobile, not fused to the underlying tissue, painless, the mucous membrane is pale pink, the color is not changed. I diagnose a stone in the duct of the salivary gland located in the membrane of the retention cyst. And I plan not only to make a small incision in the mucous membrane and remove the stone, but also to remove the entire shell of this cyst, along with all the contents and, accordingly, the stone. It is important not to injure her in order to avoid relapses.
The operation is performed under local anesthesia. Using a 15 scalpel, we make an incision into the thin mucosa. And carefully peel off the cyst shell. Soon a cystic membrane with a hard structure inside begins to protrude from the wound area. We continue to slowly and surely peel the cyst away from the underlying tissues and release it.
** – photo is not for the faint of heart (click to open):
After removing the cyst with the stone, I find another bush deeper and excise it too. It (the second cyst) was not diagnosed on an x-ray, since it was filled not with a dense substance (stone), as in the first case, but with a cloudy liquid. The picture below shows these formations with the cyst shell.
** – photo is not for the faint of heart (click to open):
removed stone
You need to look at the contents inside these cysts. I make a longitudinal incision and find a mineralized conglomerate inside a large cyst. Inside the small one there is a cloudy liquid - accumulated saliva.
** – photo is not for the faint of heart (click to open):
removed stone
Next, we inspect the wound. Antiseptic treatment with a solution of “Chlorhexidine 0.05%”, we coagulate the vessels using a laser, excise the small salivary glands located at the edges of the wound and in the field of view and apply Monocryl 5 sutures.
In the postoperative period, the following are possible: swelling due to lymph accumulation; bleeding due to the abundance of the blood supply in the sublingual area; impaired sensitivity from compression of the branches of the hypoglossal nerve by edema; painful movements of the tongue, since the operation was performed close to the root of the tongue.
Due to possible postoperative manifestations, the patient is prescribed antibacterial, anti-edematous, vascular, and analgesic therapy for up to 10 days. Cold is recommended - the first day, exclusion of vasodilating procedures and drinks, exclusion of physical activity with the head tilted down. For examination on the 2nd, 5th and 10th days. Removal of sutures after 14 days.
The patient did a great job and conscientiously followed all the recommendations. Thank her very much. This is always a huge help for the doctor!
It is imperative to remove such cysts and stones , as they will not resolve on their own!