The dental system performs the functions of breathing, swallowing, chewing and speech. It is a part of the body that changes dynamically throughout a person’s life. Its structure and functions reflect the development of the human psyche, the characteristics of his character, and behavior in society.
As the cultural level rises, people attach increasing importance to the shape of the face and the harmony of its structure.
Disorders in the maxillofacial area can be prevented by applying preventive measures and using the patterns of growth and development of the dental system.
II PERIOD - from birth to 6-9 months (before the eruption of the first milk teeth)
Prevention of dental anomalies:
- identification of congenital anomalies (cleft palate, lip) and development of a treatment plan
- rational regimen and balanced nutrition of mother and child
- breastfeeding baby
- correct artificial feeding of the child: correct positioning during feeding, preventing pressure from the neck of the bottle on the alveolar process, regulating the child’s efforts when sucking by squeezing the mother’s breast with the fingers, correct selection of the hole in the nipple, the length of the nipple and the degree of its insertion into the oral cavity, monitoring regularity swallowing
- identifying prematurely erupted teeth and deciding on their removal
Causes of anomalies
For the correct formation of a permanent bite, it is necessary to monitor the condition of the teeth in early childhood. This means that the primary units also require careful care and dental treatment, just like the elements of the permanent dentition.
If you do not remove the caries-affected milk fragment in a timely manner, then there is a high probability that the entire dentition will begin to form asymmetrically.
The remaining units will move to the empty space area. As a result, the development of the alveolar process will slow down.
At 9-10 years of age, removal of milk units is considered justified. In this case, the development of bite pathologies is not observed.
By adolescence (12-14), the risk of malocclusion after tooth extraction increases again.
It is necessary to consider in more detail what can result from premature loss or removal of primary teeth.
Loss of incisors
Early loss provokes the mixing of the fangs in an anatomically incorrect position and the tilt of the remaining elements.
Deciduous incisors perform an important function - biting off pieces of food and redistributing the chewing load between all teeth.
In addition, the absence of incisors negatively affects a person’s appearance, since they are located in the smile zone.
You should know! Orthodontists consider premature loss of primary incisors to be a serious problem. Because of this, the remaining teeth are displaced relative to the center line of the face.
Displacement of elements relative to the center line is also observed with pathological abrasion of enamel and friction of teeth against each other.
Visual signs of senile progeny and pathology treatment tactics.
Let's talk here about measures to prevent malocclusions.
At this address https://orto-info.ru/zubocheliustnye-anomalii/okklyuzii/chto-takoe-sindrom-kostena.html all the most important things about the treatment of Kosten syndrome.
Loss of primary molars
Pathology also leads to a displacement of the row relative to the center line of the face. Children with an absent first painter should undergo regular dental examinations (at least once every six months).
Loss of second primary molars
The problem can cause the permanent molar to shift and create an abnormal bite.
If it was not possible to avoid the loss of a baby tooth, then parents need to regularly show the child to an orthodontist, who will decide on the need for treatment.
The main goal of therapy in this case is to preserve sufficient space for the full eruption of the permanent element.
To do this, a specialist may recommend wearing corrective devices that prevent the remaining teeth from shifting into empty space.
From the video, learn more about the dental problems that arise with mixed dentition.
III PERIOD - from 9 months to 3 years (formation of temporary bite)
Prevention of dental anomalies:
- massage of the alveolar processes of the jaws for difficult eruption of baby teeth
- monitoring the sequence of eruption of primary teeth and their establishment in the dentition
- the use of medicated nipples that apply pressure to an overdeveloped area of the jaw
- preventing the development of bad habits: thumb sucking, constant sucking on pacifiers, placing a fist under the cheek while sleeping, etc.
- identification of habitual incorrect posture (standing, sitting, lying), postural disorders and flat feet
- therapeutic exercises, massage, orthopedic consultation
- normalization of lip closure, nasal breathing, correct positioning of the lower jaw with the help of therapeutic exercises and vestibular plates
- detection of dental anomalies. Orthodontist consultation. Dispensary observation
Timing of permanent teeth eruption
A removable bite goes through two stages in its formation:
- First phase. Celebrated between 6 and 9 years of age.
On the surface of the gums, instead of baby teeth, incisors and sixes appear. Molars may appear behind the primary teeth before they fall out. In this case, the decision to remove the mammary units is made by the orthodontist. - Second phase. Observed from 10 to 12 years of age.
At this time, children develop lateral elements - molars, premolars and canines. A sign of a correct bite is the symmetry of the lower part of the face and the sequence of teething. Due to this, the interalveolar process does not decrease.
The first permanent elements begin to function fully only 3-4 years after they appear on the gum surface.
Find out more about what a mixed dentition is in the video.
IV PERIOD - from 3 to 6 years (the period of formed temporary occlusion)
Prevention of dental anomalies:
- plastic surgery of a shortened or improperly attached frenulum of the tongue
- complexes of therapeutic exercises to normalize lip closure, position of the lower jaw and tongue at rest and during functions
- combating sluggish chewing, avoiding eating hard foods, learning to swallow correctly
- learning the correct pronunciation of individual sounds (“r”, “l”, hissing)
- planned sanitation and hygiene of the oral cavity using special-purpose products
- monitoring the depth of the incisal overlap and the shape of the dental arches
- identification of postural disorders, flat feet, teaching correct body position while standing, sitting, lying, walking
- introduction to outdoor games
Methods for correcting open bite
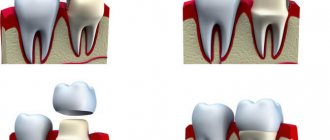
The teeth that prevent the jaw from closing are ground down. After a little grinding, the surface is polished and calcium and fluorine preparations are used for remineralization. When grinding off a significant thickness, the tooth is covered with a crown.
Teeth that lack height are augmented with crowns. In cases of insufficient height of the front teeth, veneers can be used. If all teeth are intact, then the main goal is to create occlusal contact. If a part is missing, then the task becomes more difficult. It is necessary to restore the dentition and occlusion at the same time. For this purpose, bridges and removable dentures (clasps) are used.
V PERIOD - from 6 to 9 years (initial period of mixed dentition)
Prevention and treatment of dental anomalies:
- detection of malocclusions and their orthodontic treatment
- planned sanitation of the oral cavity and regular hygiene using special-purpose products
- observation of the sequence of eruption of the first permanent molars, incisors and massage of the alveolar process
- selective grinding of unworn cusps of temporary teeth (usually canines)
- plastic surgery of a shortened or improperly attached frenulum of the tongue
- plastic surgery of a shortened or improperly attached frenulum of the upper or lower lip (if there is a diastema, three)
- removal of retained primary incisors and erupted supernumerary teeth
- identification of postural disorders, flat feet, therapeutic exercises and orthopedic consultation
- fighting bad habits of sucking and biting fingers, lips, cheeks, tongue, various objects, with habitual incorrect posture
- detection of nasal breathing disorders. Consultation with an ENT doctor. Sanitation of ENT organs. Removal of adenoids and velopharyngeal tonsils for orthodontic indications in cases of severe malocclusion
- the use of therapeutic exercises to normalize nasal breathing, swallowing, and posture
- training from a speech therapist in the correct pronunciation of individual sound phonemes
- early removal of the buds of 3 molars (wisdom teeth) at the age of 7 years
Characteristics of temporary, replacement and permanent dentition. Part 1
Over the course of a person's life, temporary and then permanent teeth emerge successively in the oral cavity. Knowledge of the anatomical structure, timing of teething, characteristics of growth and development of the jaws at different stages of the formation of the maxillofacial system, physiological occlusions is important for doctors of all specialties. This general morphological direction is basic and determines the patterns of development of the dentofacial system and reveals individual characteristics.
Timing and basic patterns of eruption of primary teeth
A newborn child's jaws contain the rudiments of 20 temporary and 16 permanent teeth of various stages of development. The lower jaw is located behind the upper jaw, and between the alveolar processes in the anterior section there is a sagittal gap of up to 10 - 14 mm. During the thoracic period, the intramaxillary formation and mineralization of temporary teeth continues, and from the 6th month the process of teething begins and a temporary bite is formed. At the same time, mineralization of permanent teeth begins. The average age of teething is the age at which the tooth erupts in 50% of children. It has been established that in a zone with a high fluoride content in drinking water, the eruption of lateral incisors, canines, and second molars begins 2-3 months later compared to a zone with a low fluoride content in drinking water. The sequence of eruption of temporary teeth on each jaw occurs in the following order: I – II – IV – III – V, and in general in the occlusion as follows: Iн – Iв – Iв – Iн – Ivн – Ivв – IIIв – IIIн – Vн – Vв. The presented order of eruption is the most typical, however, options are also possible when the child’s lateral incisors erupt first, and soon after them the central ones. Teeth usually erupt sequentially, in pairs, symmetrically. Violation of paired eruption is observed with malformations of teeth and jaws. It is considered normal when, by the end of the 1st year of a child’s life, 8 incisors have erupted, then the first molars, canines and second molars (Table 1). Table 1. Timing of mineralization, eruption and formation of teeth
However, recently, due to acceleration processes, many children begin to erupt at an earlier time - 4 or 5 months of life, so some authors propose average periods of eruption, which were determined by them as a result of their own clinical studies (Table 2).
Table 2. Anatomy of primary teeth.
Temporary teeth differ from permanent teeth in size, shape, and color (Table 3).
Table 3. Comparative characteristics of temporary and permanent teeth
Among the temporary teeth there are: incisors – 8; fangs – 4; molars – 8. The teeth are not homogeneous in their structure. This depends on the group affiliation of the tooth, on the described surface of the tooth. For convenience of description, surfaces are distinguished: vestibular, lingual, medial, distal, occlusal. The group of temporary incisors are single-rooted teeth. There are 4 incisors on each jaw: 2 medial (central) and 2 lateral (lateral), left and right, respectively. What is common in the structure of the incisors is the shape of the crown, flattened in the vestibular-lingual direction near the cutting edge. The root has a cone shape.
Rice. 1
Anatomical shape of primary teeth of the right upper jaw
Rice. 2
Anatomical shape of primary teeth of the right lower jaw.
The group of temporary canines are single-rooted teeth. There are 2 fangs on each jaw: right and left. What is common in the anatomy of these teeth is the presence of a crown that is pointed on all surfaces and the longest cone-shaped root. Group of temporary molars. These are teeth with a multi-tubercular chewing surface and several roots. Primary molars are the largest teeth in the primary dentition. The child has 8 molars: 4 molars of the upper jaw - first and second (right and left); and 4 molars of the lower jaw - first and second (right and left).
There are several systems for recording the dental formula of primary teeth.
There are three main periods in the temporary dentition: 1st period (from birth to 2.5 - 3 years) - formation of the temporary dentition; 2nd period (from 3 to 4 years) – formed temporary bite; 3rd period (from 4.5 to 5 – 6 years) – reduction (abrasion, wear) of the temporary occlusion. The period of formation of temporary occlusion. With normal development of teeth and jaws, the process of eruption of temporary teeth begins at 6–8 months (Fig. 3), lasting up to 2.5–3 years. As teeth erupt and chewing function develops, involution of those organs that previously provided the act of sucking is observed. With the eruption of the second primary molars, the first rise in the height of the bite occurs. During this period, the alveolar process actively develops, the basal part of the lower jaw thickens, its branches grow, the outlines of the mandibular canal change, the size of the mandibular angle decreases, and the relief and architecture of the lower jaw become more complex. By 2.5 - 3 years, the temporary bite is considered formed. This period lasts up to 4 years and is a stable state of the dental system. Violations in the primary occlusion can lead to various complications, both local and general. They affect the growth and development of the jaws, the eruption of permanent teeth, reduce chewing ability, and lead to changes in the shape of the hard palate. Rice. 3
The period of formed temporary occlusion has the following dental characteristics: 1. There are 20 temporary teeth, they have a pronounced anatomical shape, 2. The teeth within the dentition have close contact. The contact point is point-like, but with an increase in physiological mobility, by the end of the period of formed temporary occlusion, the contact point becomes planar. 3. the upper and lower rows of teeth have the shape of a semicircle and their midpoints coincide with each other; 4. The teeth of the upper jaw in the frontal region overlap the teeth of the lower jaw. This is explained by the greater width of the upper dental arch compared to the lower one; 5. each tooth of the upper jaw articulates with two lower ones, with the exception of the second molar, which articulates only with its antagonist - the second lower molar; 6. The distal approximal surfaces of the second temporary molars are in the same vertical plane. By the end of the eruption of primary teeth, the first stage of physiological rise in the height of the bite takes place, which begins with the establishment of contact between the first temporary molars and ends with complete eruption and correct articulatory relationships of the second temporary molars. The next period of formation of the dental system is the period of reduction of the temporary occlusion, lasting from 4.5 to 6 years. A fully formed temporary bite during this period is unstable and undergoes a number of changes. It is also called the period preceding the change in the temporary bite, or the period of “wear and tear” of the temporary bite.
Fig.4 Fig. 5
Rice. 4. Reduction of temporary occlusion (models of the jaws): a) front view, b) rear view.
Rice. 5 Correct ratio
As a result of the growth of the jaw bones in preparation for the replacement of temporary teeth with permanent (larger ones), this period is characterized by the formation of physiological gaps between the teeth (diastemas - between the central incisors and three - between the remaining teeth). The abrasion of the cusps of the chewing teeth and the cutting edges of the frontal teeth gradually increases. The physiological mobility of individual teeth to be replaced increases. The dentition lengthens. Due to the abrasion of the chewing surfaces of the lateral teeth, a medial (towards the midline) shift of the lower jaw occurs and a “direct sliding bite” is formed. In this case, the incisors contact their cutting edges, and a medial step appears in the lateral area, formed by the distal surfaces of the second temporary molars (Tsilinsky’s symptom). This relationship of teeth ensures the subsequent correct position and relationship of the first permanent molars. The spaces of primates (diastema and trema) are a reserve site for the medial displacement of the lower dentition and the subsequent unimpeded placement of permanent teeth. Wearing of teeth leads to a decrease in the height of the crowns, and a straight “sliding” bite is formed. The differentiation of the elements of the temporomandibular joints is completed, the formation of third molars, the development and mineralization of premolars and second molars continues. Towards the end of the period of “wear and tear” of the temporary dentition, the eruption of the first permanent molars begins.
Timing and basic patterns of eruption of permanent teeth
The development of permanent teeth generally resembles the development of primary teeth. Permanent molars do not have temporary predecessors, which is why they are called additional molars. All other permanent teeth are replacement teeth. During the eruption of permanent replacement teeth, destruction and loss of temporary teeth occurs, which also includes progressive resorption of the roots of temporary teeth and their alveoli (Fig. 6).
Rice. 6
Due to the pressure of the permanent tooth on the alveolus of the temporary tooth, differentiation of osteoclasts begins, which are actively involved in the processes of bone tissue resorption. The localization of the zones of physiological resorption of the roots of temporary teeth varies depending on the group affiliation of the tooth: in single-rooted teeth it is located in the area of the apex of the tooth on the lingual side, and in multi-rooted teeth - in the zone of root bifructation. The timing of the eruption of permanent teeth with the correct development of the child coincides with the time of loss of temporary teeth (Table 4). The process of temporary tooth loss occurs synchronously with the process of permanent tooth eruption. Clinically, after the loss of a temporary tooth, cusps or part of the cutting edge of the erupting permanent teeth are detected.
Table 4. Timing of eruption of permanent teeth.
The eruption of permanent teeth begins with the first permanent molar at 6 years of age. Then, sequentially at the age of 6–8 years, the central and lateral incisors erupt. At 9–10 years of age, the first premolars erupt, followed most often by the canines (10–11 years) and the second premolars (11–12 years). At 12–13 years of age, the second permanent molars erupt. Thus, by the age of 12–13 years, all temporary teeth are replaced by permanent ones. The final formation of roots is completed by 15 years. Replacement teeth have a special anatomical structure that facilitates their eruption - a conductive canal, which contains a conductive cord. The anlage of such a permanent tooth is initially located in a common bone alveolus with its temporary predecessor. It is subsequently completely surrounded by alveolar bone, with the exception of a small canal containing the remains of the dental plate and connective tissue. Together, these structures help guide the movement of the permanent tooth as it erupts.
Periods of mixed dentition
So, with the eruption of the first permanent molar, the mixed dentition begins. The mixed dentition represents a higher degree of development and differentiation of the masticatory apparatus. It is characterized by the presence of temporary and permanent teeth, which lasts from 6 to 12-14 years. The mixed bite is of particular interest to orthodontists, because at this time the most intensive growth of the jaw bones occurs, metabolic processes in bone tissue are at a high level. Therefore, timely identification of etiological factors is especially effective during the day, as is the treatment of dental anomalies themselves. However, information about the development of mixed dentition is ambiguous. So, for example, A.D. Osadchiy (1967) distinguishes two periods in the mixed dentition: 6 – 8 years – early mixed dentition and 9 – 12 years – late mixed dentition. I.L. Zlotnik (1952) also distinguishes these two periods, but with an age difference of 6 - 9 and 10 - 12 years, respectively.
Rice. 7
This allocation of periods is associated with the presence in the dentition during the period of early mixed dentition of the first permanent molar, four permanent incisors on the upper and lower jaw. And premolars and canines are in the period of late mixed dentition. At 9 years of age, the growth of the jaw bones slows down, but there is a noticeable growth of the alveolar process, associated with the eruption of permanent canines and premolars and the formation of the roots of the incisors and first molar (F.Ya. Khoroshilkina, 1999). This division takes into account the growth rate of the jaw bones and alveolar process and the level of intensity of metabolic processes in them. The eruption of the first permanent teeth (first molars) provides a second physiological rise in the height of the bite, and sagittal and transversal occlusal curves are formed. The third period of increasing the height of the bite begins at 12 years of age with the eruption of the second molar. It is accompanied by active growth of the dentoalveolar arches, which lasts from 13.5 to 15 years. During the development of the chewing apparatus in children, the mixed dentition is the most labile. The simultaneous presence in the oral cavity of temporary teeth that have lost stability due to root resorption, and permanent teeth that are at various stages of eruption and root formation, leads to a significant decrease in chewing function, leading to uneven training of the masticatory muscles, abnormal growth of the jaw bones and often the formation of anomalies dental system. During this period, both self-regulation of existing anomalies and the formation of new ones are noted. Due to the unstable condition of individual parts of the dental system and the entire masticatory apparatus as a whole, as well as the increased growth of the jaws during this period, it is necessary to use it to perform corrective orthodontic interventions. Article continues here
Authors: V.I. Kutsevlyak, A.V. Samsonov, S.V. Altunina, Yu.V. Tkachenko
VI PERIOD - from 9 to 12 years (the final period of the mixed dentition)
Prevention and treatment of dental anomalies:
- planned sanitation and training in oral hygiene using special-purpose products
- identification of dental anomalies and their orthodontic treatment
- selective grinding of unworn cusps of temporary canines and molars
- plastic surgery of the shortened frenulum of the tongue, lips (according to indications)
- removal of erupted or impacted supernumerary teeth
- identification of impaired posture, flat feet, torticollis. Therapeutic exercises and consultation with an orthopedist
- combating bad habits and incorrect postures, including during sleep
- therapeutic orthodontic gymnastics to normalize lip closure, nasal breathing, posture
- teaching proper chewing, swallowing, speech
- monitoring the sequence of eruption of premolars, canines, second molars, finger massage in this area
- rehabilitation of ENT organs
The importance of timely treatment of malocclusion
Childhood is a period when parents can become concerned about the problem of their child’s bite and solve it with “little effort” and at minimal cost. Ignored problems will result in more expensive and lengthy treatment in adolescence or adulthood.
Some consequences of malocclusion:
- inadequate chewing of food and, as a result, problems with the gastrointestinal tract;
- disruption of the respiratory system;
- uneven load when chewing can lead to accelerated “wear” and destruction of some teeth;
- possible problems with diction;
- increased risk of developing caries.
VII PERIOD - from 12 to 15 years (period of formation of permanent dentition)
Prevention and treatment of dental anomalies:
- identification of dental anomalies and their orthodontic treatment
- planned sanitation of the oral cavity, mandatory consultation with a periodontist to identify periodontal diseases and their treatment
- oral hygiene training, individual selection of hygiene and prevention products
- identification of postural disorders, flat feet, torticollis, therapeutic exercises and consultation with an orthopedist. Swimming, fitness classes
- identification of gastrointestinal dysfunctions, introduction to food hygiene, consultation with a therapist
- identification and elimination of calcium deficiency
- determination of skeletal ossification disorders and consultation with an endocrinologist
- introduction to risk factors
Price
The cost of correcting a bite is not limited to the installation of orthodontic structures. The therapy consists of successive stages, for each of which the patient is forced to pay:
- consulting a doctor and choosing the appropriate treatment method;
- diagnostic measures to identify contraindications to the procedure and measure jaw parameters;
- installation of devices selected in advance by the orthodontist;
- adjustment of orthodontic systems and their replacement;
- removal of fixed structures.
The cost of installing each orthodontic system should be considered separately:
- plates – 6,000–7,000 rubles;
- trainers – 7,000–10,000 rubles;
- mouthguards – from 15,000 rubles per set;
- braces from 16,000.
VIII PERIOD - from 15 to 21 years (completion of the formation of permanent dentition)
Prevention and treatment of dental anomalies:
- sanitation of the oral cavity, hygiene, use of individual care and prevention products
- mandatory professional hygiene
- observation by a periodontist, consultation and treatment of periodontal diseases
- identification of dental anomalies and their orthodontic treatment
- introduction to food hygiene
- elimination of calcium deficiency
- restoration of crowns of damaged teeth
- restoration of bite height, alignment of occlusion, selective grinding of teeth
- timely prosthetics
- monitoring the eruption of 3 molars (wisdom teeth) and their timely removal
- identification of incorrect habitual postures, posture disorders,
- prevention and treatment of osteochondrosis
- sports, fitness, swimming
- eliminating risk factors
- formation of useful habits and skills
- surgical treatment of severe deformities of the maxillofacial area
Is it always possible to correct an overbite?
Bite defects can be eliminated in almost any case. Orthodontic treatment eliminates not only cosmetic defects, but also allows you to maintain healthy teeth and normal functioning of the maxillofacial apparatus.
Elimination of pathology significantly improves dental hygiene and facilitates dental procedures. To find out how much it costs to correct a bite in adults, visit an orthodontist: the doctor will conduct an initial examination, give recommendations for straightening teeth and give an estimate on the cost of treatment.
PERIOD IX - from 21 to 40 years (active functions of the dental system)
Prevention and treatment of dental anomalies:
- regular sanitation of the oral cavity, compliance with hygiene rules using special-purpose products
- observation by a periodontist, treatment of periodontal diseases
- professional oral hygiene
- restoration of crowns of damaged teeth
- replacement of missing teeth using implantation and prosthetics
- removal of 3 molars
- selective grinding of teeth and elimination of traumatic occlusion
- achieving multiple contacts between teeth with various types of articulation and occlusion of the dentition
- prevention of diseases of the temporomandibular joints
- food hygiene
- elimination of calcium deficiency
- sports, fitness, swimming
- identification and elimination of risk factors
- fighting bad habits
- prevention of secondary dentofacial deformations
no images were found
Correction Methods
There are several methods for correcting malocclusion in childhood. At the initial stages of the problem, children may be shown myogymnastics, nutrition correction, or wearing removable devices.
For children under 3 years of age, soft elastic structures are recommended to prevent damage to the mucous membranes of the mouth, for example, lip bumpers.
The device helps correct pathologies of the maxillofacial apparatus and is shaped like a silicone pacifier.
It is possible to prevent the development of an abnormal bite due to the rapid loss of primary teeth with the help of removable orthodontic structures.
After 4 years, the fight against pathology is carried out according to a different scheme. To correct a pathological bite, the following are used:
Orthodontic plates
The devices are intended for children from 4 to 10 years old; they are manufactured individually depending on the parameters of the patient’s jaw.
The shape of the plate resembles an overlay covering units of both jaws and a system of fastenings. Due to the fixing element, the force of pressure on the teeth changes.
Orthodontic plates perform a number of important functions:
- prevent further development of existing defects;
- move incorrectly located units to their normal position;
- adjust the parameters of the palatal wall.
The effect of the structures can only be achieved with continuous wear , so parents need to ensure that the child does not remove the plates from the mouth. At night, the device should also be in the child’s mouth.
Trainers
Most often they are installed from the age of 7. Trainers are made of dense silicone using computer modeling.
The following types of trainers are used in pediatric dentistry:
- periodontal – redistribute the chewing load between all teeth;
- for braces – prescribed to older children and used to correct deficiencies in the masticatory apparatus;
- retainers – prescribed after the main course of treatment with braces to consolidate the results obtained.
In 90% of cases, treatment with trainers gives positive results. In addition, after wearing the devices, no additional installation of corrective structures is required.
The success of therapy largely depends on the child’s ability to wear the device for the prescribed time.
Let's figure out together how the pacifier affects the bite, and how to avoid problems.
In this article we will tell you how to correct a crooked jaw.
Here https://orto-info.ru/zubocheliustnye-anomalii/chelyustey/lechenie-rezko-vyirazhennyih-kompaktosteotomii.html read what compactosteotomy is and to whom the operation is indicated.
Mouthguards
The structures are made from hypoallergenic materials . Mouth guards can be standard or custom-made to fit the patient's jaw. In the latter case, the effect of using the devices will be more noticeable.
The devices are sold in sets. Each of them is designed to last several weeks of wear. During this time, the teeth have time to change their position to install the next aligner.
Thus, the dentition gradually returns to its normal anatomical position. The treatment period ranges from six months to 2 years.
You should know! Orthodontic plates and aligners are removed during meals and when brushing teeth.
Structures require regular hygienic care. They are washed under running water and treated with antiseptic solutions.
Braces
The optimal time for installing structures is 9-10 years. Braces are a thin arch attached to clasps, which, in turn, are fixed to the teeth. The arc controls the force of pressure on the elements.
Depending on the material, braces are divided into ceramic, metal, sapphire, plastic, and combined.
Teenagers may be offered lingual systems, which are installed on the inside of the dentition.
These braces are less noticeable, but require longer basic correction times and more careful maintenance.