The formation of teeth is a complex step-by-step process that begins in the first weeks of intrauterine life. Thus, by the time of birth, the baby has the rudiments of 20 primary and 16 permanent teeth inside each jaw. But, like all stages of development, teething in children under one year and older occurs differently. Some endure this period relatively calmly, others are capricious and sleep poorly. Why this happens and how to understand that the baby is cutting teeth, we will tell you further.
Size of modern human teeth
Over more than two million years, the size of teeth gradually decreased due to the transition to eating soft and processed foods. The first transformations affected the fangs - in primates they were larger and more strongly advanced relative to the rest of the row. The interdental spaces have disappeared, the size of the front teeth has become smaller. Refusal of raw meat led to a decrease in the chewing load and a narrowing of the jaw, as a result of which there was no room left for the “eights”. Now wisdom teeth are considered atavism and are often subject to removal.
Caring for baby teeth
You need to take care of your teeth immediately after teething. Moms do it first. For adults, special finger brushes have been created that are convenient for cleaning teeth from plaque, but so far without toothpaste. When the baby learns to rinse his mouth and spit, they move on to brushing with children's toothpaste without fluoride (this can be done earlier if the tube indicates that the toothpaste is from 0 years). So, gradually, the child will form a useful habit of caring for the oral cavity.
Another important reason for caring for teeth from infancy is that it affects the formation of permanent teeth and bite. For example, caries of a temporary tooth can transfer to the germ of a permanent one. And early loss (before 5 years) of a baby tooth will lead to uneven dentition in the future. If the molar does not begin to grow in time, the adjacent baby teeth will move and fill the resulting space.
How are tooth sizes determined?
To determine the size of a person’s permanent teeth, the calculation tables of Wetzel and V.L. Ustimenko with average standards and permissible deviations are used. However, an experienced dentist is able to independently identify the anomaly during a visual examination or by applying the formula for the ratio of the height and width of the natural crown. During diagnosis, the specialist takes into account the patient’s face shape and height. For example, with a wide jaw, the size of teeth exceeding the norm is not a pathology.
To determine the size of the root canal, there are also tables that indicate the average distance from its apex to the cutting edge or cusp of the tooth surface. The longest is the root of the canines - about 26 millimeters, the root canal of the incisors is 21 - 23 millimeters, and the size of the roots of the chewing zone and premolar teeth ranges from 19 to 22 millimeters.
Teeth size for prosthetics
It is especially important to preserve and, if necessary, restore the natural size of teeth during prosthetics, so as not to disrupt the bite and the full functioning of the dental system. The size of the crown is selected by the dental technician, focusing on neighboring or teeth of the same name, monitoring the correct closure of the rows and adjusting the prosthesis during installation.
Determining the size of artificial teeth with complete edentia is carried out by measuring the distance between the corners of the mouth using a special ruler - it corresponds to the width of the six front teeth. And the segment from the edge of the gum to the smile line is equal to the height of the crown. For example, during implantation it is necessary to correctly calculate not only the parameters of the orthopedic design, but also the size of the dental implant. It should be equal in length to the real root, but the choice of titanium rod parameters depends largely on the volume of the jaw bone tissue.
Proportional ratio of teeth sizes
In most cases, specialists determine the proportions of a tooth by correlating its height and width. A result of about 0.75 is considered ideal. The most accurate diagnosis is carried out through the use of formulas.
- Gerlach's formula.
The method is based on the proportional ratio of the sizes of the front teeth and dental units of the chewing zone. The width of the crowns of the upper central incisors should correspond to the width of the four lower incisors. The canine, two premolars and one molar of both jaws are normally equal to each other. The width of the lateral part of the dentition is 10 mm greater than the width of the anterior segment. - Pon's formula.
The distance between the first premolars is equal to the sum of the widths of the four incisors multiplied by 100 and divided by 80, and the distance between the first molars is the sum of the widths of the four incisors multiplied by 100 and divided by 64. - Corkhouse formula.
The length of the segment from the midline to the first molar of the upper jaw should be 2 mm greater than the same distance on the lower jaw.
Restoration of the anatomical shape of the anterior group of teeth
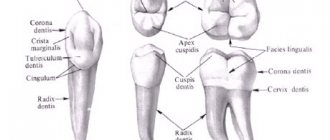
The dentofacial system is the initial section of the human digestive tract. With the help of the dentition of the upper and lower jaws, food is crushed into small components, forming, when wetted with saliva, a volume of food bolus. In addition to performing this function, the teeth in the dentoalveolar system, together with the facial muscles, also take an active part in the articulation of speech sounds. All this creates a single, functional integrity of the body, where the anatomical shape of the teeth (morphology) of the upper and lower jaw is one of its important and integral parts.
The anatomical shape of the teeth in the dentition, of all parts of the human dental system, is most directly related to the functional purpose of the digestive tract. Many anatomical and spatial connections transform the dentition into an interconnected deep-spatial composition, which, in addition to the function of cutting, tearing, holding and crushing food, also carries a great aesthetic aspect. Strict mathematical proportions determine anatomical points, shape filling lines, edges, and planes in the teeth of the upper and lower jaw, the distortion of which, even to a slight extent, leads to a violation of aesthetics and functional occlusion and speech diction. If you analyze the construction of the vestibular and palatal surfaces of the frontal group of teeth, you will notice that the teeth in the dentition form a certain sequence. According to E. Levin’s description, the ratio of the sizes of the vestibular surface of the frontal teeth (central incisor to lateral incisor; lateral incisor to canine, etc.) is a proportion in the digital ratio 1: 0.618, which corresponds to the proportion of the “golden section” (from the materials of the Esthetic dentistry magazine ) . Each subsequent tooth corresponds in a certain proportion to the previous one. A slight distortion of the relationship or change in the size of just one mesial or distal facet can completely change the perception of the entire dentition
anterior group of teeth. Before starting work, a dentist or dental technician must thoroughly study the main anatomical landmarks of the dentition.
The vestibular surface of the anterior group of teeth must meet the following parameters (Fig. 1)
From the palatal surface, the construction of the anterior group of teeth looks like this (Fig. 2)
Knowledge of anatomical landmarks (form filling lines, edges and planes in the dentition) can greatly simplify the work. But it should also be noted that recreating the shape of the teeth in the dentition requires constant monitoring from all points of view. A dentist or dental technician is required to have the ability to generally perceive the volume of a tooth, a sense of the vestibular and palatal surface as a whole.
When working, for example, on a veneer of a central incisor, it is necessary to analyze the work of each stage from all planes at once. In addition to the general view of the vestibular surface, a schematic “coordinate system” (the general anatomical structure of the construction of teeth in the dentition) should always be in front of the eyes, which can significantly simplify the task of constructing the shape of a specific tooth.
Let's take a closer look at the structure of the front teeth.
CENTRAL INCISERS (teeth 11 and 21).
The upper central incisors are powerful single-rooted teeth with a crown flattened in the vestibular-palatal direction. Of all the anterior teeth of the upper and lower jaw, the central incisors are the most stable teeth in terms of reduction. The shape of the crown of the upper central incisor can take various variations, but three of the most common ones can be noted.
This is a rectangular shape, when the parallel side edges resemble the shape of a rectangle, a triangular shape, with the side edges converging towards the neck, and an oval shape, when the side edges form an approximate oval shape and the greatest width of the crown is in its middle third. The approximal surfaces of the central incisors often differ from each other in their content. The medial surface has a more rigid, vertical line that forms a straight, sometimes acute angle with the line of the cutting edge of the crown, and the distal surface has a rounded surface with a pronounced fracture line in the shape of the lateral edge and a blunt, mostly rounded distal angle
The volume of the root in relation to the central axis of the tooth is shifted in the distal direction and has three planes: vestibular, medial and distal. On the surface of the tooth root, from two apraximal surfaces, one can notice two small hollows, indicating the formation of the volume of the crown from two components of the primary principles, the volume of the “facet” of the vestibular surface and the volume of the palatal tubercle.
The line of the incisal edge of the crown usually has a beveled surface in the distal-palatal direction, with a thin line of dentin often visible. If we consider the shape of the central incisors, with a non-erased surface (in young patients), then on the surface of the cutting edge of the crown, you can see three protruding tubercles (lobes), each of which is divided on the vestibular surface by a weakly defined longitudinal hollow. From the side of the cutting edge, you can also notice an uneven filling of the volume of the crown from the medial and distal surfaces, called the mesial-distal rotation of the crown or a sign of enamel curvature. From the medial surface of the tooth, the volume of the crown seems much thicker than from the distal surface, which creates the impression of a helical turn of the crown around the root and makes it difficult, at the time of restoration, to correctly position the incisor in the dentition. The development of the medial-distal spread usually has a gradual filling from the medial to the distal edge, but sometimes it can take the form of thickening of a separate lobe, not the medial one, but, for example, the central one. Then the general ratio of volumes is violated, and the sign of the medial-distal turn will be changed.
On the vestibular surface, in addition to two vertical hollows dividing the volume of the crown into three lobes, on the upper third of the tooth crown, fracture lines of the lateral edges are formed, forming a barely noticeable drop-shaped volume on the vestibular surface of the incisor (vestibular volume). This shape on the surface of the crown of the central incisors is clearly visible from the distal side, but on all other teeth of the dentition, this shape formation is very pronounced (especially in the canines and premolars) both from the distal and medial surfaces.
The structure of the palatal surface of the crown combines the volume of the palatal tubercle and the central plane into a single form. On the medial and distal sides, the crown is limited by two lateral volumes of the medial and distal edges. The degree of development of these volumes varies from a barely noticeable form to a strongly pronounced volume. With a strong development of the lateral edges, two powerful “rollers” are formed on the palatal surface of the incisor crown, giving the shape of the incisor crown a “scoop-shaped” shape. The lateral volumes, in a similar situation, can converge at the point of the equator line, uniting the medial and distal edges and forming a “blind fossa” point on the palatal surface in the area of the upper third of the tooth crown. With a normal degree of development, the medial and distal ridges dock with the volume of the palatine tubercle, forming a smooth transition of volumes along the fracture line of the lateral edges. The shape of the palatine tubercle is a powerful volume, from which two additional tooth-like volumes extend towards the incisal edge, turning into thin, sometimes barely noticeable ridges on the central surface. On the surface of the crown there are usually two faces on the mesial and distal sides, however, various variations are possible when the number of faces changes and they differ from each other in size. If the volumes of the lateral faces on the surface of the crown of the central incisor are strongly expressed, then the shape of the central faces can be combined with the lateral faces, forming a scoop-shaped volume of the crown.
On the approximal surface, the structure of the central incisor forms a smooth transition from the vestibular surface to the palatal surface. At the moment of intersection, two mutually directing lines form the line of the anatomical neck of the tooth, the plane of the triangle of the gingival papilla and the volume of the proximal surface of the contact points. The line of the anatomical neck has a characteristic bending shape. From the vestibular and palatal surfaces, the volume of enamel extends significantly higher than from the medial and distal surfaces, which creates more dense contact with the volume of gum surrounding the crown. The degree of bending of the line of the anatomical neck of the tooth can take various variations, but on the medial side the bend is usually more pronounced than on the distal side. If a vertical line is drawn through the point of the apex of the bend of the line of the anatomical neck of the tooth, then in relation to the line of the cutting edge of the crown and the point of the root apex, this line will be in a more vestibular direction. In their daily practical work, in addition to clinical tasks, dentists constantly have to deal with the possibility of improving the aesthetic shape of the patient’s teeth and the problem of correct placement of teeth in the dentition. The points, edges and lines of filling the form presented for study in this section (“the coordinate system of the main anatomical landmarks”) allows dentists and dental technicians to operate with the form, deliberately change the volume in a non-standard situation, during rotation, crowding diastemas and tremata, as well as determine the correct construction of the form at the time of retrusion and protrusion of teeth. Knowledge of the deep-spatial system for constructing interlocking lines of form filling helps to change the proportional relationships of the teeth in the dentition without violating their basic structure of construction. For example, identically given proportions of the central incisors (height A and width B) can change their external perception by changing the content of just three main landmarks: the mesial and distal edges, the equatorial point of the vestibular surface and the mesial-distal inclination and the direction of the mesial and distal angle crowns
In one of the main types of fine art, sculpture, there are two ways to recreate a form. The first is modeling (alternate collection of material in small portions until the volume is completely completed), the second is sculpting (cutting off excess volumes of material to the original form). The method of step-by-step construction involves recreating the volume of the tooth using sculpting, since any excess of accumulated material leads to the wrong way of doing the work, to overkill, and subsequently to grinding off the excessively accumulated material with a bur. Initially, incorrectly collected material interferes with the integral perception of the tooth shape and the analysis of the correct construction of the volume. Therefore, the reconstruction of the tooth crown should be built in small portions along anatomical points and lines of filling the form, taking into account knowledge of the principles of bionic construction.
If we try to break down the structure of the construction of the central incisor into supposed stages, then we can propose the following method for restoring the central incisor
STEPS OF CONSTRUCTION OF THE VESTIBULAR SURFACE OF THE CENTRAL INCISER (VINEER).
Recreating the shape of the vestibular surface of the central incisor using a step-by-step construction method can be carried out in four stages: 1-formation of the volume at the point of the equator line of the vestibular surface. 2- construction of the medial and distal edges; 3- reconstruction of the vestibular plane. 4 - formation of vestibular volume. This construction is typical for wax modeling when creating diagnostic models and temporary structures
FIRST STAGE. (formation of volume at the point of the equator line of the vestibular surface.).
Using the guide lines, the line of the axis of the root of the tooth being restored, and the line of the secondary inclination of the dentition, we determine the point of the equator line of the vestibular surface of the incisor. At the intended point, on the surface of the tooth crown, we collect the first portion of material. We distribute the collected material from the base of the crown (the line of the anatomical neck of the tooth) to the points of the fracture line of the lateral edges of the vestibular surface, dividing the volume of material into two planes, forming in the area of the point the equator line of the crown, guide lines for the medial and distal edges. (Fig. 8).
The volume of collected material must correspond to the main guidelines:
1) - Points of the equator line of the vestibular surface. 2) - The central line of the root of the tooth being restored. 3) - a given angle b forming the mesial-distal filling of the crown
/explanation/.
a) If we consider the shape of the crown of the central incisor from the cutting edge, we can see that the mesial-distal filling of the crown is formed from three different volumes (lobes) in terms of filling (Fig. 9.) The mesial lobe A has a larger volume than the distal lobe C Therefore, the recruitment of the initial portion of material of the vestibular surface (at the point of the equator line) should be made taking into account the mesial-distal filling of the crown. The line at its intersection with straight AB creates an angle b that determines the medial-distal filling
b) Simultaneously with the point of the equator line, the point of “secondary crown inclination” is formed.
If we analyze the construction of the shape of the tooth crown from the approximal surface, we can see that the point of the equator line of the vestibular surface is at the intersection of two lines. The central line of the root and the line passing through the cervical plane of the tooth crown. The angle of intersection of the two lines should be approximately 30 degrees. The intersection of the central line of the root with the plane of the lower third of the crown approximately corresponds to an angle of 10 degrees. The vestibular surface constructed in this way determines
the correct functional load of the crown, makes it possible to hit a food bolus at the point of primary and secondary inclination of the crown. The formed angle prevents injury to the gums, helping to provide additional massaging. (Fig.10).
The construction of the vestibular surface in this way is characteristic not only of the anterior group of teeth, the lines of primary and secondary inclination of the crown are clearly expressed on the vestibular surface of almost all teeth of the lateral incisors, canines, premolars and molars.
SECOND STAGE (Construction of the medial and distal edges)
After determining the point of the equator line, we determine the direction of the medial and distal edges of the crown. We apply longitudinal portions of the material to the vestibular surface, determining the main portions of the crown volume (Fig. 11).
Using a spatula, we form two planes in each of the lateral volumes, forming guides for the medial and distal edges. The central lobe is slightly flattened. The main landmarks for the lateral volumes at this stage are the medial and distal edges of the adjacent central and lateral incisors (teeth 12 and 21). For the central lobe, the guideline is the filling of the vestibular surface of the adjacent central incisor.
THIRD STAGE (recreation of the vestibular surface)
After determining the three main guide volumes of the vestibular surface of the central incisor, we produce an additional set of material, filling the central part of the crown in small portions. Using a small amount of material, we collect the lateral edges of the vestibular surface of the central incisor.
The main guidelines for the correct selection of material at this stage are the medial and distal edges of adjacent teeth and the vestibular surface of the adjacent incisor.
On the lower part of the vestibular surface of the crown, two small portions of material are collected, giving a smooth transition to the cutting edge. A thin layer of material is collected at the base of the cutting edge to complete the formation of the cutting edge of the crown (Fig. 13)
At this stage, the general process of forming the vestibular surface of the incisor using the method of step-by-step material collection has been completed. The next stage in the formation of the vestibular surface is processing, which is necessary to give the crown an additional anatomical shape and remove, if necessary, excess material.
FOURTH STAGE (formation of the vestibular volume of the crown)
The final formation of the vestibular surface of the central incisor occurs at the last fifth stage during the formation of refraction lines of the lateral edges and longitudinal hollows during processing and polishing of the veneer. Processing must be done very restrainedly, constantly paying attention to control landmarks, anatomical points and lines of filling the shape of adjacent teeth.
After correcting the basic shape, during processing it is necessary to pay attention to the formation of fracture lines of the medial and distal edges that form the volume in the upper third of the crown (Fig. 15). With enough experience, this feature can be easily formed during “sculpting”... On the central incisor this volume will not be expressed as significantly as on the canine or premolar, but recreating this volume is very important, especially from the distal edge. The shape of the vestibular volume gives the tooth a finished appearance and forms a deep-spatial connection between the vestibular surface and the palatine surface. After the final stage of recreating the vestibular surface of the central incisor, a shape is formed that corresponds to the main anatomical points and filling lines.
STEPS OF CONSTRUCTION OF THE PALATAL SURFACE OF THE CENTRAL INCISOR.
The construction of the palatal surface of the central incisor can be carried out in five stages:
1-formation of volume at the point of the equator line; 2 - construction of the medial and distal edges. 3-filling of the central plane. 4-recreation of serrated volumes
FIRST STAGE. (Formation of volume at the point of the equator line.).
On the palatal surface of the dentition we find the guide of the points of the equator line. We determine the central line of the root of the tooth being restored. At the intersection of the line, we select a point on the equator line of the palatal surface and form the first portion of the material.
From the collected material we recreate the volume of the palatal tubercle of the crown. From the point of the equator line of the palatal surface of the crown, we divide the accumulated volume into additional planes, forming guide lines for the lateral edges of the palatal surface of the incisor. The general boundary of the material collection should be in the area of three points. Two points located on the fracture line of the lateral edges and the point of the anatomical neck of the tooth crown (Fig. 17).
The main landmarks at this stage are the points of the equator line of the palatal surface of the dentition, the volume of the palatal tubercle of the adjacent incisor.
SECOND PHASE. (Construction of the medial and distal edges).
From the points of the fracture lines of the lateral edges to the line of the cutting edge of the crown, we collect two longitudinal lateral volumes. (lateral ridges) From the formed lateral volumes we form the medial and distal edge of the palatal surface of the central incisor. (Fig. 18)
THIRD STAGE (filling the palatal plane)
Using a small amount of material between the volumes of the medial and distal edges to the line of the incisal edge of the crown, we gain the volume of the palatal plane
When recreating the palatal surface at this stage, it is necessary to pay attention to the formation of the cutting edge of the crown, which is visible on the palatal surface of the central incisor.
FOURTH STAGE (formation of two tooth-shaped ridges of the palatal surface)
Along the fracture line of the lateral edges on the palatal surface of the central incisor, we collect two volumes. From the collected volumes we form two tooth-shaped edges of the palatal surface (Fig. 19). These volumes are not always clearly expressed and have individual characteristics.
At this stage, the construction of the palatal surface can be considered complete; final processing should be carried out without disturbing the formed anatomical shape. Recreation of the palatal surface is as important as the vestibular one, since errors in its formation lead to a number of undesirable consequences and dysfunction when the incisal path of maintaining the upper and lower dentition is disrupted.
GENERAL STRUCTURE OF THE CENTRAL INCISER CONSTRUCTION.
This section considers the reconstruction of the shape of the central incisor as a single overall volume, simultaneously with the vestibular, palatal and proximal surfaces. This construction technique gives a general idea of the shape of the tooth in the dentition and its correct position at the time of occlusion. The method can be used not only by dental technicians but also by dentists to teach the step-by-step construction of a tooth shape from modeling wax and a light-curing composite. The construction of the central incisor can be carried out in eight stages.
FIRST STAGE (recreation of the volume of the tooth stump)
The construction of the crown of the central incisor should proceed from a pre-formed “initial” volume. If the volume of the stump is formed for further restoration of the tooth crown from multilayer plastic or light-curing composite on the surface of the tooth stump, it is necessary to build a volume of mamelons from dentin, which will give the volume of the tooth crown an internal color fullness. (Fig. 20) To build a tooth crown from modeling wax, recreating the internal volume of mamelons is not required. The main guideline for correctly constructing the volume of a tooth stump is the anatomical shape of adjacent teeth.
SECOND STAGE (determination of points of the equator line on the vestibular and palatal surface).
To place a tooth crown in the dentition, it is necessary to correctly determine the points of the equator line on the vestibular and palatal surface. On the vestibular surface, the point of the equator line is located at the intersection of the line of the central axis of the root and the guide passing through the points of the equator line of adjacent teeth. On the palatal surface, the point of the equator line is located at the intersection of the central line of root filling and the main guideline of the points of the equator line; at the designated points on the vestibular and palatal surface we collect the first two portions of material. The collected volumes are divided into two additional planes, forming the guide lines of the lateral edges of the palatal tubercle and the vestibular volume.
The main guidelines at this stage will be: 1) Guide points of the equator line of the vestibular and palatal surfaces. 2) Line of the cutting edge of the dentition 3) Angle forming the medial-distal filling of the vestibular surface. (Figure 21.)
THIRD STAGE. (Formation of the lateral surfaces of the crown).
From two apraximal surfaces (from the neck of the tooth stump to the line of the cutting edge of the crown) we collect two lateral volumes. Using a small tool from the collected material, from a point along the line of the anatomical neck of the tooth and from a point towards the line of the cutting edge, we form the lateral planes of the triangle of the gingival papilla and the surface of the apraximal contact points.
On the side of the line of the cutting edge of the crown, at this stage of construction, four approximate points are formed (two points of the equator line on the vestibular and palatal surfaces and two points of contact points of the apraximal surfaces), which determine the main landmarks in the direction of placement of the tooth crown in the dentition.
From the contact points along the line of the cutting edge of the dentition, we collect the next portion of material and form the line of the cutting edge of the crown. Using collected portions, we recreate the future contour of the vestibular surface of the central incisor from the vestibular surface (Fig. 22).
Main landmarks: 1) Two proximal points of the medial surface of adjacent incisors. 2) Contour of the vestibular surface of the adjacent central incisor. 3) Line of the incisal edge of the dentition
FOURTH STAGE (Construction of the medial and distal edges of the vestibular surface.)
From the point of the equator line to the cutting edge of the crown, we define two lines of the medial and distal edges of the central incisor. Along the designated lateral lines and the central line of the vestibular surface, we collect three longitudinal volumes of material. (Three beats). We divide two lateral volumes into planes, forming medial and distal edges. (fig23)
Along the medial and distal edges, at the point of the equator line, we line up the lateral plane of the vestibular surface.
FIFTH STAGE. (Formation of volume at the point of the equator line of the palatal surface.) /volume of the palatal tubercle/.
From the points of the line of the anatomical neck of the palatal surface to the points of the fracture line of the lateral edges, we collect a portion of material. We form the volume of the palatal tubercle. (Fig. 24.)
The reference point at this stage will be the volume of the palatal cusp adjacent to the central incisor.
SIXTH STAGE (Formation of the medial and distal edges of the palatal surface)
From the points of the fracture line of the side edges to the line of the cutting edge of the crown, we assemble two side bolsters. Using a smoother, we divide the collected volume of material into two planes and form the medial and distal edges of the palatal surface. (Fig. 25.)
SEVENTH STAGE. (Construction of the lateral ridges of the palatal surface.)
From the fracture line of the lateral edges to the points, we use two portions of material to form the volumes of the two lateral ridges and the edges of the palatal surface (Fig. 28).
The reference point for construction at this stage will be the anatomical shape of the palatal surface of the adjacent incisor.
At this stage, recreating the shape of the central incisor using the step-by-step construction method can be completed (the “sculpting” stage). For the final formation of the tooth volume, additional processing and polishing is required, completing the ninth stage. ("sculpting" stage
EIGHTH STAGE. (Formation of fracture lines of the lateral edges of the vestibular and palatal surfaces.)
During the final processing of the tooth shape, in addition to eliminating possible excess material, attention should be paid to the formation of fracture lines in the shape of the lateral edges of the vestibular and palatal surfaces. From the palatal surface, these lines form the volume of the palatal tubercle (Fig. 29); from the vestibular surface, the form of “vestibular volume” is formed (Fig. 30). The formation of these lines is typical for any group of teeth. On the vestibular surface, the formation of fracture lines of the lateral edges is more pronounced on the premolar canines and demarcations. In incisors, this shaping is also present, but it is more pronounced on the distal side. When processing the shape of the crown of the central incisor, it is necessary to pay attention to the structure of these volumes.
The proposed method for constructing the crown of the central incisor gives a general idea of the anatomical shape of the tooth. After acquiring certain theoretical knowledge, practical experience, and the ability to determine the main landmarks for the correct placement of teeth in the dentition, the number and stages of operations at the time of constructing the shape of the tooth can be individually changed.
Normal and deviations in tooth sizes
All dental units of the same name have approximately the same height and width, except for the central (medial) incisors. The size of the front teeth of the upper jaw is normally slightly larger than that of the lower jaw. The height of the crown of the upper central incisors varies from 9 to 12 millimeters, width - from 8 to 9 millimeters. The lower teeth are similar in height, but are about 5 millimeters wide. The size of a person's wisdom teeth does not differ from the parameters of other molars. The table below shows the average width of dental crowns in millimeters.
| Upper jaw | Lower jaw | |
| Medial incisor | 8.5 mm | 5.3 mm |
| Lateral incisor | 6.5 mm | 6 mm |
| Fang | 7.6 mm | 6.7 mm |
| First premolar | 6.7 mm | 6.8 mm |
| Second premolar | 6.4 mm | 7 mm |
| First molar | 9.4 mm | 10 mm |
| Second molar | 9.4 mm | 10.2 mm |
Anomalies in the size of human teeth can be congenital or acquired and are accompanied by malocclusion, impaired chewing functions and an unaesthetic appearance of a smile. The most common deviations are macrodentia and microdentia.
Timing of teething in children
On average, the first teeth in healthy children appear at 5–6 months. But sometimes it happens that someone has a white bump visible at 4 months, and someone smiles with a toothless mouth even at 8-12 months. And this is not a deviation from the norm. According to studies by a number of authors, the timing differs depending on the region of residence, race, and gender of the child. For example, children in the southern regions develop teeth a little earlier than those in the north. The formation of temporary teeth is also influenced by the following factors:
- heredity;
- maternal toxicosis in the second and third trimester of pregnancy;
- prematurity;
- artificial feeding;
- quality of drinking water;
- hypothyroidism and other endocrine pathologies;
- infectious diseases;
- weakened immunity;
- rickets.
It is impossible to speed up the timing and influence the sequence of teething in children. The only thing parents can do at this time is to alleviate the baby’s condition if he is restless and in pain (more on this below).
Macrodentia
The tooth size exceeds the norm by more than 2 millimeters. Pathology occurs due to the fusion of two rudiments or the main and supernumerary teeth during the period of formation. The cause of macrodentia can be endocrine diseases, metabolic disorders or heredity. There are five types of pathology:
- localized - one or two teeth are significantly larger than the rest;
- generalized - the entire dentition differs in size from the other;
- isolated - enlargement of one medial incisor;
- absolute - the size of the teeth of both jaws exceeds the norm;
- relative - excessive growth of the upper or lower incisors.
Signs of teething
How can parents understand that their child is teething? The easiest way to find out about this is by the child’s changed behavior. He sleeps worse and is capricious. He loses his appetite (may completely refuse to eat). But similar symptoms can be caused by other reasons. Therefore, the most obvious sign can be considered swelling of the gums (a small red bump appears on it, which parents can feel rather than see).
The child's changed behavior is associated with the movement of the tooth in the jaw. It seems to tear the gums from the inside, which explains the unpleasant sensations: itching, burning and pain. To remove them, the child can scratch his gums, pull various objects into his mouth, and bite. You cannot stop this behavior; you just need to replace inappropriate objects (for example, toys) with special teethers, the purpose of which is to help relieve the unpleasant consequences of teething.
It is because of the unpleasant sensations that the child may begin to refuse food, especially hot food (increases the pain). A light massage of the gums may help, which should be performed before feeding. It will relieve some of the itching and pain.
During teething, the baby's temperature can rise to 38º, but not higher. Until the teeth appear, parents should pay as much attention to the child as possible, distracting him from unpleasant sensations. This will help the baby get through a difficult time for him.
Microdentia
The size of teeth in microdentia is less than anatomical standards. The list of reasons for deviation includes exposure to radiation, premature removal of a baby tooth, narrow jaw, and infectious diseases. There are several types of anomalies:
- isolated - a single violation affecting the lateral incisors;
- relative - the teeth are of normal size, but look smaller due to the enlarged jaw, as a result of which interdental spaces and diastema are formed;
- generalized - the defect covers a group of teeth.