Central lower incisor
Average age of eruption: 6-7 years
Average age of root formation: 9 years
Average length: 20.7 mm
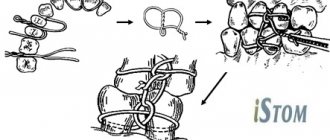
Narrow and flat in the labial-lingual direction, the lower central incisor is the smallest adult tooth. Radiologically it is visible in only one projection and thus appears more accessible than it actually is. The crown, narrow in lingual projection, has a limited area for access. For gentle access formation, a fissure bur and a spherical bur No. 2 are used. The access cavity should be oval and performed on the lingual side.
The lower central incisor often has two canals. One study reported that 41.4% of mandibular central incisors studied had two separate canals, of which only 1.3% had two separate apical foramina [1]. After completing the access formation, the doctor must examine the tooth cavity to identify an additional canal. Endodontic treatment failures in the lower incisor area are most often associated with an unidentified canal, usually in the lingual location. To create conditions for the straight entry of endodontic instruments into the additional canal, access can be expanded in the incisal direction.
There is a great danger of perforation of the vestibular wall, but it can be avoided if the doctor remembers that it is almost impossible to perforate in the lingual direction, since the bur axis is in contact with the incisal edge. The slit-like lumen of the canal is so common that it can be considered a normal variant, and this requires special attention when cleaning and shaping.
Lateral perforations and pulp anatomy will be discussed in an illustration of the lower second molar.
Lateral lower incisor
Average age of teething: 7-8 years
Average age of root formation: 10 years
Average length: 21.1 mm
Very similar to the lower central incisor, so access cavity preparation follows the same principles.
Their similarity can cause rare but serious errors. Hasty installation of a rubber dam, identical fillings and carelessness can lead to preparation of the access cavity on the wrong tooth. This error can be prevented by marking the vestibular surface of the tooth with a felt-tip pen before applying the rubber dam.
Trauma, periodontal disease, carious lesions and malocclusion can lead to obliteration of the canal. When moving apically to identify the orifice, great care must be taken to prevent unnecessary destruction of the crown and root. Labial perforations were discussed in Illustration IX. If the bur is not oriented along the long axis of the tooth, there is a risk of lateral perforation. The situation becomes more complicated with the traumatic loss of an anatomical crown. Without anatomical landmarks, a lateral perforation can be easily made when moving in a coronal direction. To prevent this, access is carried out without a rubber dam so that the root can be palpated.
Lateral perforation with endodontic files and Gates-Glidden burs is facilitated by the presence of slit-shaped canals with a narrow, hourglass-shaped cross-section. To avoid vertical fracture along the approximal root wall, minimal expansion and preparation of the space for the abutment pin is indicated.
Apical curves and accessory canals are common in the lower incisors.
Size of modern human teeth
Over more than two million years, the size of teeth gradually decreased due to the transition to eating soft and processed foods. The first transformations affected the fangs - in primates they were larger and more strongly advanced relative to the rest of the row. The interdental spaces have disappeared, the size of the front teeth has become smaller. Refusal of raw meat led to a decrease in the chewing load and a narrowing of the jaw, as a result of which there was no room left for the “eights”. Now wisdom teeth are considered atavism and are often subject to removal.
Mandibular canine
Average age of teething: 9-10 years
Average age of root formation: 13 years
Average length: 25.6 mm
The canine of the lower jaw is more powerful and significantly wider than the incisors in the mesial-distal direction. It rarely causes treatment problems. The atypical form with two roots can be problematic, but is rare.
The access cavity is oval and can be expanded in the incisal direction to facilitate vestibular-lingual access. In the cervical region the canal is oval, in the middle third it is rounded. To completely clean its walls, directed instrumental action is necessary.
If there are two roots, one of them will always be easier to instrument. The other canal must also be opened and funnel-shaped in accordance with the first to prevent dentine filings from entering it and impairing access. Pre-bending the instruments during the initial approach will allow the clinician to walk along the walls of the buccal or lingual root until the tip of the instrument enters the orifice. Once a difficult-to-reach canal has been identified, every effort must be made to shape and create a funnel-shaped orifice to keep access open.
Forms and functions of human tooth types:
Incisors.
The incisors are located at the front of the mouth. These teeth have sharp edges and are adapted for cutting food into small pieces. Humans have eight incisors, four in the upper jaw and four in the lower jaw.
Fangs.
Fangs. They are located in the “corners” of the dental arches. They are characterized by a sharp, elongated and pointed surface. Their main function is to grab and tear food (tough foods such as meat). Humans have four fangs: two on the upper jaw and two on the lower jaw.
First lower premolar
Average age of teething: 10-12 years
Average age of root formation: 12-13 years
Average length: 21.6 mm
Often considered a mystery to endodontists, the mandibular first premolar, with its two canals separating at different levels of the root, can be very difficult to machine.
The crown consists of a well-developed buccal cusp and a small or almost non-existent lingual enamel protrusion. The approach is performed buccally from the central sulcus and directed along the long axis of the root to the central cervical region. The oval-shaped pulp chamber is opened using fissure burs with a cutting apex and elongated spherical burs No. 4 or 6. In teeth with one canal, the pulp cavity in the neck area has an almost circular cross-section, and in teeth with two canals it is oval.
One study reported that “at least 23% of first mandibular premolars have a second or third canal”[17]. The canals can split almost anywhere in the root. Due to the lack of direct access, cleaning, shaping and filling these teeth can be extremely difficult.
In a recent study, Vertucci [13] showed that the first lower premolar has one canal at the apex in 74.0% of cases, two canals in 25.5% and three canals in the remaining 0.5% of cases.
Classification and frequency (%) of canal types in first and second lower premolars
By Vertucci, F. J. Am. Dent. Assoc. 97:47, 1978.
Restoration of a maxillary lateral incisor affected by aplasia
Aplasia of both maxillary lateral incisors was reported in a 22-year-old female patient.
After orthodontic treatment, the previous dentist installed dental implants, one at a time, in the area of 12 and 22 teeth. The patient came to our clinic with symptoms of peri-implantitis in the area of the previous 22 tooth (photos 1, 2). During the initial visit, impressions were also taken of the maxilla and mandible, and a single temporary prosthesis was fabricated immediately prior to surgery to maintain occlusal stability and restore the defect after implant removal.
Photo 1
Photo 2
Surgical procedure
The implant in the area of the 22nd tooth was removed, and all inflamed tissue was treated through careful curettage. Using X-ray diagnostics, the presence of a multi-wall bone defect was confirmed (photos 2, 3).
Photo 3
Eight weeks after removal of the implant, the bone defect was augmented using an autologous bone block removed from the angle of the lower jaw, as well as graft bone material (botiss cerabone) and a collagen membrane (botiss jason). Six months after reconstruction of the defect, an all-ceramic implant of reduced diameter was installed (diameter: 3.3 mm / length: 10 mm), which was argued by tissue deficiency in the mesio-distal direction. On the vestibular side, during implantation, additional augmentation was performed with bone chips collected from the zygomatic area (photo 4, 5).
Photo 4
Photo 5
The healing process proceeded without disturbances (photo 6).
Photo 6
In order to protect the implant, a temporary prosthetic structure was fixed to adjacent teeth.
Prosthetics stage
To form an adequate soft tissue profile, a temporary composite crown was fixed to a Straumann support cap. After this, a temporary crown made using CAD technology was additionally used (photo 7). After 16 weeks, impressions were taken to create the final ceramic crowns (Figure 8). The radiograph taken after treatment shows the position of the implant and the prosthetic structure fixed on it (photo 9).
Photo 7
Photo 8
Photo 9
conclusions
In conditions of scarce bone tissue, and therefore limited space for implant installation, it is quite difficult to achieve adequate and aesthetic results of complex dental rehabilitation, and the concept of staged treatment could be used. The choice of the all-ceramic Straumann implant with a reduced diameter of 3.3 mm and a macro-/micro-rough surface was quite justified in this clinical situation. In addition, the patient herself expressed a desire that metal supports not be used during treatment, which could compromise the aesthetic result of the treatment by shining through the gum. Guided bone regeneration was carried out according to a standard protocol. Major contributions to the implementation of the treatment protocol described in this article were made by Michael Gahlert, Munich (Germany) and Dr. Stefan Rohling, Basel (Switzerland).
Author: Florian Thieringer (Basel, Switzerland)
Second lower premolar
Average age of teething: 11-12 years
Average age of root formation: 13-14 years
Average length: 22.3 mm
The second lower premolar, which is very similar in crown shape to the first premolar, has a less complex root.
Its crown has a well-developed buccal cusp and a much better formed lingual cusp than on the first premolar. The access is made slightly oval, wider in the mesial-distal direction. They begin to form access in the central sulcus with a fissure bur with a cutting apex, and then expand and form the contour of the burr hole with spherical burs No. 4 and 6.
Researchers reported that only 12% of mandibular second premolars studied had a second or third canal [17]. Vertucci [13] also showed that second premolars had one apical foramen in 97.5%, while only 2.5% of the teeth examined had two foramina.
An important circumstance that should not be forgotten is the anatomical location of the mental foramen and the vessels and nerves passing through it. Due to the proximity of these structures, an acute inflammatory process in the area of the lower premolars can cause temporary paresthesia. The exacerbation of the pathological process in this area is more severe and resistant to conservative treatment than in other areas.
Text of the book “Fundamentals of clinical dental morphology: a textbook”
3.1.3. Mandibular medial incisor
The medial incisor of the mandible is the smallest among the incisors. The mesial-distal size of the crown is significantly less than its height when compared with other incisors. The vestibular-lingual size of the root greatly exceeds its mesial-distal size. Signs of lateralization are weakly expressed.
In vestibular and lingual norms
the shape of the crown is close to an irregular quadrangle with a predominance of the height of the crown over the mesial-distal size (Fig. 15).
Rice. 15. Medial incisor of the lower jaw, right.
a – vestibular norm; b – language norm.
The cutting edge is often relatively smooth. In unworn teeth, there are tubercles on the cutting edge (the medial and distal ones are more pronounced than the middle ones). The crown angles practically do not differ from each other (the sign of the crown angle is not informative).
The approximal contours of the crown weakly converge towards the neck of the tooth. The most prominent points on the contours of the contact surfaces of the crown are located near the border of its occlusal and middle thirds.
The enamel-cementum border is curved towards the root evenly and approximately equally in both the vestibular and lingual norms.
The contact contours of the crown without sharp boundaries transform into the corresponding contours of the cone-shaped root. Often the transition from the medial and distal contours of the crown to the same contours of the root is more noticeable on the distal side. The apical part of the root is slightly curved distally.
The relief of the vestibular surface is weakly expressed. On the vestibular surface of the crown of unworn teeth there are two vertical grooves, separating three vertical ridges that pass into the tubercles of the cutting edge.
On the lingual surface of the crown there are marginal ridges, which are often separated from each other by a median ridge. The marginal ridges, belt and tubercle of the tooth are less developed than those of other incisors. In the lingual norm, both of its contact surfaces are visible on the root.
In medial and distal norms
the shape of the crown, like that of all incisors, is close to a triangle with the base in the area of the neck of the tooth (Fig. 16).
Rice. 16. Medial incisor of the lower jaw, right.
a – medial norm; b – distal norm.
The line of the occlusal contour is straight, short and slightly beveled in the direction from the vestibular to the lingual surface, towards the base of the crown.
The occlusal contour becomes vestibular near the IVS (often on the lingual side of the IVS). The vestibular contour of the crown near the border of the cervical and middle thirds is convex (equator of the tooth).
The lingual contour of the crown at the site of localization of the lingual tubercle is curved in the lingual direction, and along the remaining length to the incisal edge is slightly curved towards the USV.
The line of the enamel-cementum border is convex towards the cutting edge, the most protruding point is located near the USV. The enamel-cement junction in the distal norm has a smaller amplitude of curvature than in the medial one.
The transition of the vestibular and lingual contours of the crown to the corresponding contours of the root is clearly visible. The vestibular contour of the root is usually convex; the lingual contour can be either convex, straight or even concave. The apex of the cone-shaped root is located near the USV.
The approximal surfaces of the tooth have little relief. In the distal norm, the vertical groove of the root is more pronounced than in the medial one. this fact can be used as an additional feature when determining whether a tooth belongs to the right or left side of the dental arch.
In occlusal norm
the shape of the crown is close to an irregular quadrangle with rounded corners in place of the largest convexities of the vestibular and lingual contours and their transitions into each other (Fig. 17, a).
Rice. 17. Medial incisor of the lower jaw, right.
a – occlusal norm and section at the level of the base of the crown; b – tooth cavity.
The vestibular contour forms a weakly defined medial-distal slope. The conical contour of the crown has a greater curvature than the vestibular one.
In horizontal sections, the shape of the root approaches an irregular oval with concave medial and distal contours and a sharp predominance of the vestibular-lingual size over the medial-distal one.
Tooth cavity
resembles its external contours (Fig. 17, b). The cavity of the crown in the upper part is slit-like narrowed in the vestibular-lingual direction, and in the area of the base of the crown, without noticeable boundaries, it passes into the root canal.
In the middle part of the root, the canal often bifurcates into vestibular and lingual, with the subsequent connection of these branches in the apical part. On transverse sections, both channels have a rounded shape. The lingual canal is located close to the lingual surface of the root.
Anatomical options.
In
the vestibular (lingual) norm,
the shape of the crown often looks like a rectangle with a sharp predominance of the height of the crown over the mesial-distal size. There are incisors whose crown shape is close to triangular, oval or trapezoidal.
The cutting edge is often straight, but can be rounded to varying degrees. The severity and number of tubercles of the incisal edge vary. The approximal contours of the crown often converge towards the neck, but can be almost parallel to each other. The crown angle sign is usually uninformative.
The point of greatest convexity of the enamel-cement junction is most often located along the USV, but can be displaced distally. More often, the curvature of the enamel-cementum border in the vestibular and lingual norms is approximately the same, but sometimes it can be more pronounced on the lingual side.
On the vestibular surface of the crown, as a rule, there are three vertical ridges, of which the medial and distal ones are more pronounced. The number of ridges and their severity may vary. There are incisors with a uniformly convex or flattened vestibular surface of the crown.
On the lingual surface of the crown, between the barely noticeable marginal ridges, a median ridge may extend from the tubercle of the tooth. Depending on the severity of the ridge, the central part of the lingual surface of the crown can be concave, flat or convex.
The transition of the approximal contours of the crown to the corresponding contours of the root is often more pronounced on the distal side. In the vestibular (lingual) norm, the direction of the root apex varies.
In the medial (distal) norm
the line of the vestibular contour of the crown varies from slightly convex to straight. The contour of the crown can be smooth, convex or concave. The cutting edge of the crown can be located along the USV or be shifted to the lingual side.
The vestibular contour of the root can be smooth or convex, the lingual contour can be smooth, convex or concave.
The height of the tooth varies from 16.9 to 26.7 mm, while the height of the crown is 6.3-11.6 mm, the height of the root is 7.7-17.9 mm.
The mesial-distal size of the crown between the contact points ranges from 4.4 to 6.7 mm, the neck - from 2.7 to 4.6 mm. The size of the crown in the vestibular-lingual direction in the equator region ranges from 4.8 to 6.8 mm, in the cervical region - from 4.3 to 6.3 mm. 3.1.4.
Lateral incisor of the lower jaw The lateral lower incisor is larger than the medial one, has a wider crown and a more massive root. To determine whether a tooth belongs to the right or left side of the dental arch, all three main signs of lateralization are applicable.
In vestibular and lingual norms
the shape of the crown is close to triangular with a rounded apex at the enamel-cement border (Fig. 18).
Rice. 18. Lateral incisor of the lower jaw, right.
a – vestibular norm; b – language norm.
The occlusal contour of the crown is often uneven and turns into approximal contours, forming crown angles of different sizes. The mesial angle of the crown is less than the distal one (a sign of the angle of the crown).
The approximal contours of the crown converge from the cutting edge towards the neck of the tooth. The mesial contour of the crown slopes more towards the USV than the distal one. The most prominent points of the approximal contours of the crown, through which the equator line passes, are located near the border of the occlusal and middle thirds of the crown.
The enamel-cementum border is curved towards the root, and on the lingual side, as a rule, to a greater extent than on the vestibular side. The points of greatest convexity of the enamel-cementum border in both norms are located near the USV.
The transition of the crown contour to the root contour is more noticeable on the distal side than on the medial side. The root is longer than that of the mandibular medial incisor, with a clearly visible sign of root position.
The relief of the vestibular surface is weakly expressed. In unworn teeth, on the vestibular surface there are two shallow vertical grooves separating the enamel ridges, which turn into the tubercles of the cutting edge. The medial and distal ridges are usually more noticeable than the middle one. The vestibular surface of the root is smooth.
On the lingual surface of the crown, marginal ridges are visible, which are connected to each other near the belt. In the area of the cervical third of the crown there is a tooth tubercle. The lateral surfaces of the root weakly converge towards the lingual side.
In medial and distal norms
the crown has a shape close to the shape of a triangle, the most acute angle of which corresponds to the cutting edge (Fig. 19).
Rice. 19. Lateral incisor of the lower jaw, right.
a – medial norm; b – distal norm.
The occlusal contour has a slight bevel in the lingual direction. The line of the occlusal contour passes into the vestibular and lingual contours of the crown, most often on the lingual side of the USV. The vestibular contour is curved, its most prominent point is located near the border of the cervical and middle thirds of the crown. The lingual contour of the crown is convex towards the lingual side at the site of the lingual tubercle and curved towards the USV from the upper part of the lingual tubercle to the occlusal contour.
The line of the enamel-cementum border is convex towards the occlusal contour. The most prominent point of the enamel-cementum border is located approximately along the USV. The amplitude of the curvature of the enamel-cementum border in the medial norm is, as a rule, greater than in the distal norm.
The transition of the contours of the crown to the corresponding contours of the root is weakly expressed.
The root is conical. The root apex is located near the USV. The vestibular contour is often convex; the lingual contour can be either convex, straight or concave in shape. On the distal surface of the root, the vertical groove is deeper than on the medial surface. This sign can be used as an additional criterion for determining whether a tooth belongs to the right or left side of the dental arch.
In occlusal norm
the shape of the crown, as well as that of the medial incisor of the lower jaw, is close to an irregular quadrangle with rounded corners in the places of greatest curvature of the vestibular and lingual contours and in the places of transition of these contours (Fig. 20, a).
Rice. 20. Lateral incisor of the lower jaw, right.
a – occlusal norm and section at the level of the base of the crown; b – tooth cavity.
The medial contour of the crown is somewhat longer than the distal one.
The degree of curvature of the lingual contour is more pronounced than the vestibular one. The point of greatest convexity of the lingual contour is displaced distally.
The sign of crown curvature is more noticeable than that of the medial incisor of the lower jaw (medial-distal slope of the vestibular contour).
On horizontal sections, the root has the appearance of a laterally “compressed” oval with a more pronounced concavity of the distal contour.
Tooth cavity
resembles its external contours, it is more voluminous than that of the medial lower incisor (Fig. 20, b).
In the upper part, the cavity of the crown is slit-like narrowed in the vestibular-lingual direction and smoothly passes into a narrow root canal.
The root canal, as a rule, is single, flattened in the medial-distal direction.
Anatomical options.
In
the vestibular norm,
the severity of the enamel ridges and the degree of convergence of the contact contours of the crown to its base are variable.
In the language norm
the size of the marginal ridges varies. Sometimes the lingual surface is smooth. The root apex is often directed distally. Less commonly, the root is straight or curved to the medial side.
In contact standards
The vestibular contour of the crown can be either convex or smooth. The lingual contour can be curved to varying degrees.
The root canal in its middle part may bifurcate.
Tooth height varies from 18.5 to 26.6 mm.
In this case, the height of the crown is 7.3-12.6 mm, the height of the root is 9.4-18.1 mm. The mesial-distal size of the crown between the contact points ranges from 4.6 to 8.2 mm, the neck - from 3.0 to 4.9 mm. The size of the crown in the vestibular-lingual direction in the equator region ranges from 5.2 to 7.4 mm, in the cervical region - from 4.3 to 6.8 mm. Test tasks
The largest tooth in the incisor group is:
a – medial incisor of the upper jaw;
b – lateral incisor of the upper jaw;
c – medial incisor of the lower jaw;
d – lateral incisor of the lower jaw.
On the upper jaw, the smaller ones are:
a – medial incisor;
b – lateral incisor.
On the lower jaw, the largest in size are:
a – medial incisor;
b – lateral incisor.
The convexity of the enamel-cement border towards the cutting edge is most pronounced:
a – on the medial surface of the incisors;
b – on the distal surface of the incisors.
Vertical root grooves on both lateral surfaces are pronounced:
a – at the medial incisor of the upper jaw;
b – at the lateral incisor of the upper jaw.
Signs of tooth lateralization are weakly expressed:
a – at the medial incisor of the upper jaw;
b – at the lateral incisor of the upper jaw;
c – at the medial incisor of the lower jaw;
d – at the lateral incisor of the lower jaw.
The lingual tubercle is more developed:
a – at the medial incisor of the upper jaw;
b – at the lateral incisor of the upper jaw.
Bifurcation of the root canal is most typical:
a – for the medial incisor of the upper jaw;
b – for the lateral incisor of the upper jaw;
c – for the medial incisor of the lower jaw.
In the medial incisor of the lower jaw, the vertical root groove is more pronounced:
a – on the medial surface of the root;
b – on the distal surface of the root.
A sign of root position is the deviation of the root apex:
a – to the medial side;
b – to the distal side;
c – to the vestibular side; d – to the lingual side.
A sign of crown curvature is:
a – slope of the vestibular surface of the crown in the medial-distal direction;
b – slope of the vestibular surface of the crown in the distal-medial direction;
c – roundness of the distal corner of the crown.
Answers to test tasks:
1
A;
2
b;
3
b;
4
a;
5
B;
6
in;
7
b;
8
in;
9
b;
10
b;
11
a.
3.2. Group of fangs
Fangs (dentes canini) –
single-rooted teeth with a sharp “tearing cusp” (main cusp) of the occlusal contour. They are located in the dental arch between the incisors and premolars (third position) and are designed to “tear” food.
Humans have four permanent canines:
– canines of the upper jaw
(right and left);
– fangs of the lower jaw
(right and left).
What is common in the anatomy of the fangs is the presence of a cone-shaped crown, pointed on all surfaces, and the longest root.
The canine of the upper jaw is larger than the canine of the lower jaw.
The approximal surfaces of the upper canine converge to a greater extent towards the neck of the tooth, and the lingual cusp is better defined than that of the antagonist of the same name. This makes it easy to determine whether a tooth belongs to the upper or lower jaw. The canines show all the main signs of lateralization. 3.2.1.
Maxillary canine The maxillary canine has a crown pointed on all surfaces, the longest root and well-defined signs of lateralization.
In vestibular and lingual norms
the shape of the crown is close to pentagonal (Fig. 21).
Rice. 21. Maxillary canine, right.
a – vestibular norm; b – language norm.
The occlusal contour of the main tubercle consists of two segments extending from its apex, which is located somewhat mesially from the USV. These segments form an angle between themselves that is close to a right angle. The mesial segment of the occlusal contour is less extensive than the distal one (an important additional sign of tooth lateralization). The place of transition of the occlusal contour to the distal one is closer to the base of the crown than the place of transition of the occlusal contour to the mesial one.
The approximal contours of the crown sharply converge towards the USV, while the distal contour, as a rule, deviates more towards the USV than the mesial contour.
The enamel-cementum border is curved towards the root apex. The degree of curvature of the enamel-cementum border is more pronounced in the lingual norm. The most prominent point of the enamel-cementum boundary in the vestibular norm is located near the USV. On the lingual side, the same point is often displaced mesially from the USV. The transition of the contact contours of the crown to the corresponding contours of the root is more pronounced on the distal side.
The apex of the cone-shaped root of the tooth, as a rule, is located distally from the USV (a sign of root position).
On the vestibular surface of the crown, two vertical depressions are visible, separating three enamel ridges. The most pronounced is the median ridge, which is located from the main tubercle to the neck of the tooth. Of the other two vertical ridges, the mesial one is better expressed than the distal one. The vestibular surface of the root is relatively smooth.
Along the edges of the lingual surface of the crown there are marginal ridges, which are separated by depressions from the median ridge. The depression between the median and distal ridges is more noticeable than the depression between the median and mesial ridges.
The median ridge runs from the main tubercle to the lingual. The prominent tubercle is located near the enamel-cementum border and determines its sharp convexity towards the apex of the tooth root. The marginal ridges converge towards the lingual tubercle. The mesial and distal surfaces of the root converge in the lingual direction and are clearly visible from the lingual side. The distal surface of the root is somewhat convex, the mesial surface is flattened.
In mesial and distal norms
the shape of the crown resembles a triangle with the base located at the neck of the tooth (Fig. 22).
The occlusal contour is rounded and passes into the vestibular contour of the crown on the vestibular side of the IVD.
The vestibular contour of the crown is convex, its most prominent point is located in the cervical third.
Rice. 22. Maxillary canine, right.
a – mesial norm; b – distal norm.
The shape of the lingual contour is determined by the size of the lingual tubercle and the median ridge. In the area of the lingual tubercle, the lingual contour is usually convex. The contour of the median ridge can be convex, straight or concave from the main tubercle to the lingual.
The enamel-cementum border is curved towards the occlusal contour, more so on the mesial side than on the distal side. The point of greatest convexity of the enamel-cement border is located, as a rule, near the USV.
The transition of the vestibular and lingual contours of the crown to the corresponding contours of the root in the mesial and distal norms is well expressed.
The vestibular contour of the root is often convex, and the lingual contour is concave in the apical third and convex throughout the rest. The root apex is located near the USV.
The distal surface of the root is somewhat convex, the mesial surface is flattened. Both approximal root surfaces have vertical grooves. On the distal surface of the root, the groove is less noticeable than on the mesial surface.
In occlusal norm
the shape of the crown resembles an irregular quadrangle with rounded corners (Fig. 23, a).
The points of greatest convexity of the vestibular and lingual contours of the crown are approximately equally distant from the projection of the “tearing tubercle”. The point of greatest convexity of the vestibular contour is shifted to the mesial side. The sign of crown curvature is clearly visible. The curvature of the lingual contour, as a rule, is more pronounced than the vestibular one, with the point of greatest convexity located near the USV.
Rice. 23. Maxillary canine, right.
a – occlusal norm and section at the level of the base of the crown; b – tooth cavity.
In a horizontal section, the shape of the root approaches the shape of an irregular oval, elongated in the vestibular-lingual direction. Along the lateral contours of the root there are depressions, of which the mesial one is more pronounced.
Tooth cavity
matches its external shape. The cavity of the crown is pointed towards the main tubercle and has indentations towards the corners of the crown (Fig. 23, b). From the neck, the cavity of the crown gradually narrows and passes into a relatively wide root canal.
Anatomical options.
The shape of the crown of the upper canine is variable. The shape of the crown of the canine can resemble incisors or premolars.
In the vestibular (lingual) norm
the mesial and distal segments of the occlusal contour (slopes of the “tearing cusp”) often form an angle close to a right angle. There are variants of the tooth crown with an acute angle of the occlusal contour. In cases where the angle formed by the slopes of the main tubercle is close to unfolded, the canine is shaped like an incisor. On the distal slope of the “tearing tubercle” there may be an intermediate (additional) tubercle, from which a weakly defined enamel ridge extends onto the vestibular surface. The degree of convergence of the contact contours of the crown changes towards the neck of the tooth. The amplitude of the curvature of the enamel-cementum boundary is variable.
On the lingual surface
The severity of the median ridge, which largely determines the relief of the lingual surface, varies. In the presence of a wide, rounded and well-developed median ridge, the lingual surface becomes convex, giving the crown a conical shape. With a weak expression of the median ridge, the lingual surface is somewhat concave in the occlusal and middle thirds of the crown and is shaped like the lingual surface of the incisors. The lingual tubercle may be split into two fragments. The grooves separating the ridges and tubercles of the lingual surface are usually well defined. Often the groove separating the distal marginal ridge bifurcates in the middle third of the crown, limiting the so-called triangular fossa. Sometimes the grooves extending from the distal marginal groove (second order) cover a triangular elevation, which passes into the intermediate tubercle of the distal slope of the main tubercle [9].
In contact norm
vary the degree of convexity of the vestibular and lingual contours of the crown. The tip of the lingual tubercle may be close to the enamel-cementum junction or reach the middle of the lingual contour. The point of greatest convexity of the enamel-cementum border can be located along the USV or be shifted vestibular from the USV.
The amount of curvature of the root apex to the distal side is variable. The root sometimes “splits” into vestibular and lingual. The root canal is often deviated distally. There are variants of curvature of the root canal in the vestibular direction.
The height of the tooth ranges from 20.0 to 38.4 mm, while the height of the crown is 8.2-13.6 mm, the height of the root is 10.8-28.5 mm. The mesial-distal size of the crown between the contact points ranges from 6.3 to 9.5 mm, the neck - from 3.6 to 7.3 mm. The size of the crown in the vestibular-lingual direction in the equator region ranges from 6.7 to 10.7 mm, in the cervical region - from 6.1 to 10.4 mm.
First lower molar
Average age of teething: 6 years
Average age of root formation: 9-10 years
Average length: 21.0mm
The mandibular first molar erupts earlier than other permanent teeth and most often requires endodontic treatment. It usually has two roots, but sometimes three roots are found, with two canals in the mesial root and one or two canals in the distal root.
The distal root is easily accessible for endodontic cavity preparation and mechanical treatment.
The doctor can directly see the opening(s) of the canal. The distal root canals are wider than those of the mesial root. Sometimes the mouth is wider in the buccolingual direction. This indicates the presence of two channels or a slit-like channel with a complex network-like configuration that can complicate cleaning and shaping.
The mesial roots are usually curved, with the greatest curve in the mesiobuccal canal. The orifices of the canals at the bottom of the pulp chamber are usually clearly separated from each other and located buccally and lingually relative to the upper tubercles.
The tooth often undergoes extensive filling. It almost always experiences a strong chewing load, so the coronal pulp cavity can be obliterated. It is easiest to identify the mouths of the distal canals.
Then the mouths of the mesial canals are found, which will be located in the above locations in the same horizontal plane.
Since the mouths of the mesial canals lie under the mesial tubercles, they may not be detected during normal cavity preparation. In this case, to determine their location, it is necessary to remove the hard tissue of the tubercle or filling. During access preparation, overhanging molar cusps need to be ground down [15]. Remember that this tooth, like all other lateral teeth, after endodontic treatment requires complete restoration of the entire occlusal surface area. Therefore, to identify anatomical landmarks and orifices, it is better to make a wider access cavity than to skip one or more channels for the sake of “sparing” preparation, which may cause failure.
Skidmore and Bjoradal [11] found that approximately one third of the mandibular first molars examined had four root canals. If there are two canals, “they either remain separate with separate apical foramina, or unite and form a common apical foramen, or communicate with one another by transverse anastomoses partially or completely... If the tooth, instead of the usual triangular shape, had a more rectangular shape, this would allow better vision and explore a possible fourth canal in the distal root.”
In the area of bifurcation of the roots of the lower molars there are several orifices of additional canals [9]. They are usually impossible to clean and shape, and are rarely visible except incidentally on radiographs when they are filled with root cement or heated gutta-percha during treatment. It would be correct to assume that if irrigation solutions tend to clean the canal from protein decomposition products, then the area of root bifurcation in the pulp chamber must be thoroughly cleaned (remove denticles, etc.) so that the solutions can reach the small mouths of the canals.
All infected dentin, leaking fillings, and pulp denticles must be removed before endodontic treatment begins. It is recommended to completely cover the cusps with a restorative structure after endodontic treatment.
Functions of the dental system:
- Chewing is the main function of the teeth and dentofacial system. Chewing is the first stage of the digestion process.
- Aesthetics. The dental system affects the appearance of the face. Teeth also play an important aesthetic role. The position, shape and shade of teeth have a significant impact on the formation of a person’s personality.
- Pronunciation. Teeth help us pronounce words correctly as they play an important role in the pronunciation of consonants. Missing teeth (especially the upper front teeth) or an incorrect bite can somewhat impair normal speech.
Second lower molar
Average age of teething: 11-13 years
Average age of root formation: 14-15 years
Average length: 19.8 mm
The crown is somewhat smaller in size than the first molar, and the more symmetrical second lower molar is characterized by a close arrangement of roots. The roots gradually converge distally and have closely spaced apices.
Exposure is made at the mesial portion of the crown with access extending only slightly distal to the central sulcus. After trephination of the cavity with a fissure bur with a cutting apex, an elongated ball-shaped bur is used to expand it until free access is achieved. The distal root angles often allow for a smaller opening than the lower first molar.
Particular attention should be paid to the shape of the mouth of the distal canal. A narrow oval orifice indicates the presence of a slit-like lumen in the distal canal, which requires more careful treatment.
All carious tissue, leaking fillings and denticles should be removed and replaced with a suitable temporary filling prior to endodontic treatment.
The lower second molar is most susceptible to vertical fractures. After preparing the access, but before starting endodontic treatment, the clinician should examine the floor of the pulp cavity using fiber optics. For mesial-distal crown or root fractures, the prognosis is extremely unfavorable.
To avoid vertical fractures after endodontic treatment, it is necessary to completely cover the cusps with a restorative structure.