By length
This is a classification according to Kurlyandsky. According to this criterion, pathology is divided into the following types:
- Localized. Individual units or groups of them are erased. It is diagnosed mainly from the front side, for example, with a deep bite. Local compensation occurs due to the appearance of a hypertrophied alveolar process.
- Generalized. All rows are involved, the height of the bite changes significantly. Whether abrasion will be compensated by the body is determined by its individual characteristics.
Physiology is to blame for everything
To begin with, let's say that all the causes of tooth wear can be divided into two large classes - physiological and pathological.
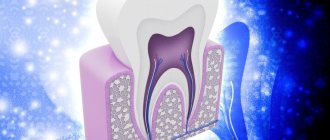
The first reason appears immediately after the final eruption of baby teeth - and this is a natural process. In children, the incisors, cusps on the canines and molars gradually wear away, and by the age of 6 years, the depth of wear down to the dentin can be observed. In the future, until the age of 14, when the teeth are finally replaced by permanent ones, abrasion of the dentinal layer of the first teeth is sometimes noted. Severe abrasion is diagnosed when the entire upper part of the tooth disappears or the cavity becomes visible.
In general, due to physiological characteristics, teeth adapt to stress during the process of wear. Without dangerous overloads, the work of the entire dental system is adjusted; contacts between teeth change the angle from point to plane, so that the closure of the jaws is more physiological.
If the changes affect only the enamel, there is nothing to worry about. But if dentin begins to participate in the process of abrasion, this is a reason to consult a doctor.
Treatment methods
Treatment of pathological tooth wear may include therapeutic and orthopedic techniques. In the first case, there are two options:
- Drug therapy (includes the application of gels and solutions, the use of special toothpaste).
- Restoration (special filling material is used).
Orthopedic treatment involves the manufacture and installation of onlays, dentures or crowns, which restore the normal appearance and functionality of teeth.
Currently, dentists do not agree on the timing of initiation and specific treatment methods in different situations. Most often, drug treatment is used in patients in the early stages of the disease, when the teeth are not yet seriously damaged. For more severe pathology, restorative and orthopedic treatment is indicated.
How is pathology determined?
Only a specialist can detect a violation during tooth wear. Of course, the general picture among the population is taken as the norm, but the doctor also takes into account individual factors:
- general condition of the enamel;
- presence or absence of exposed dentin;
- work of the temporomandibular joint;
- condition of the mucous membranes of the tongue and cheeks;
- degree of severity of nasolabial folds;
- sensitivity of the masticatory muscles.
It is interesting that in addition to all the individual characteristics, the doctor is interested in the sound with which the jaws close. A sharp, clear and short sound indicates that there are no problems. A long-lasting sound accompanied by a squeak indicates deficiencies in the functioning of the TMJ or problems with the nervous system.
You can understand that teeth are subject to increased abrasion by the first sign - increased sensitivity. It is sharper when the upper hard layer of enamel is significantly abraded.
Why does tooth wear occur?
What determines the level of tooth wear?
Wearing of teeth throughout life is a natural process that occurs to one degree or another in every person. The level of abrasion of hard dental tissues depends on various factors - the general state of their health, genetic predisposition to various diseases, the quality of food and water quality, sufficient intake of essential minerals, and also work in certain hazardous industries, for example, in the chemical industry, can speed up the process erasing the enamel.
Modern and classic classification of abrasion
In modern Russian practice, the most widespread and popular is the Bushan classification of abrasion, which distinguishes:
✔
physiological abrasion (only enamel is affected);
✔
transitional (enamel + dentin suffers);
✔
pathological abrasion (dentin is damaged).
The benefit of the classification is that, in addition to the degree of pathology, it considers the surfaces (vertical, horizontal) that have undergone changes, the prevalence of the disease and the tooth sensitivity accompanying the process.
As for the types of pathological abrasion, the classical classification was developed by A. G. Moldovanov and L. M. Demner. According to their data, the rate of abrasion is 0.402 mm per year.
- The first degree of abrasion
is achieved by the age of 25-30 and is characterized by smoothing of the cusps and cutting edges of the teeth. - The second degree of abrasion
is observed in patients aged 44-50 years and is expressed in the abrasion of the enamel. - The third degree of abrasion
is noted if by the 50th anniversary the enamel limit has been reached and 10 pairs of chewing teeth have been preserved.
Stages of dental destruction: when are consultation and diagnosis necessary?
By degree of destruction:
- Stage 1: there is a smooth smoothing of the tubercles on the enamel and the cutting edges of the teeth;
- Stage 2: tooth enamel is completely erased, the destruction process reaches dentin (the inner part of the tooth);
- Stage 3: the size of the part of the tooth located above the gum and clearly visible is only two-thirds of the norm;
- Stage 4: the crown of the tooth is completely destroyed and falls to the level of the gum.
Due to increased abrasion, the most unimaginable patterns may appear on the surface of tooth enamel, indicating damage to the enamel in the vertical, horizontal directions, in the form of dots, etc.
- Promotion
Dental treatment under anesthesia
Promotion for sedation in Moscow!
If you experience: — Severe stress during dental treatment — Fear of the sound of dental instruments — Time-limited visits to the dentist
old price
12 000 ₽
price
5 900 ₽
Free consultation RUB 5,900 for 30 minutes
Limited offer. Sign up for a free consultation. There are contraindications, consultation with a specialist is required.
- Promotion
Teeth whitening ZOOM
Promotion for teeth whitening in Moscow!
As a gift: - Prof. Oral hygiene – Whitening care set with individual trays
old price
40 000 ₽
price
19 900 ₽
Free consultation Sign up for a free consultation. There are contraindications, consultation with a specialist is required.
Causes of pathological abrasion
There are several main reasons for the development of abrasion pathology, and in the first place among them are bad human habits. For example, the habit of gnawing seeds, holding small objects in the mouth (pins, cloves, pipe mouthpiece), love for foods with high acidity may well become catalysts for the process.
Often the cause of increased abrasion is diseases: bruxism, diseases of the gastrointestinal tract, nervous, cardiovascular, endocrine systems, from the side of the TMJ - malocclusion. The cause may also be improper dental treatment - an incorrectly manufactured orthopedic design can provoke severe abrasion of the antagonist tooth.
Sometimes the cause of pathology may be the chosen profession. Some employees of the metallurgical, cement, granite industries, and representatives of the mining workshop suffer from increased abrasion.
Multidisciplinary approach to the treatment of anterior tooth wear: a step-by-step protocol
Taking into account an accurate risk profile, as well as predicting outcomes, are critical in planning and implementing dental treatment. Such treatment, in its essence, should foresee a minimal risk of complications, be promising and provide a stable long-term effect. In addition, open communication and collaboration with both the patient and other dental professionals is essential for clinicians to achieve treatment goals and desired results.
In this case, the patient sought help with long-existing wear on his front teeth. Although he had understood the essence of the problem for 10 years, he never had sufficient motivation for treatment until he got married and until his wife noticed the appearance of his smile. During a comprehensive dental examination, it was determined that severe wear of the anterior group of teeth was the result of their incorrect position. Functional diagnostics revealed limited masticatory excursion. Given that the back teeth had not been restored, an orthodontic approach was recommended as a possible option in the comprehensive treatment to improve the appearance of the smile. Careful planning with the orthodontist was aimed at correcting the position of the teeth and their alignment, improving the functionality of the dentition and providing sufficient space to restore the length of the clinical crowns.
Case review
A 42-year-old man sought treatment for severely worn front teeth and problems with his smile (Figure 1 and Figure 2). The nature of wear on the front teeth of the upper and lower jaws was not physiological for his age. The size of the central upper incisors was only 6 mm vertically. The back teeth were diagnosed with signs of erosion, and although they required restoration, their level of wear was minimal. The patient's medical history did not contain any information regarding this disease.
Photo 1. View of the patient’s face and smile before treatment: the patient has difficulty demonstrating the level of his teeth.
Photo 2. View of the maximum tubercular-fissure contact of the antagonist teeth: severe abrasion of the anterior teeth.
Diagnostic criteria, risk assessment and prognosis
Periodontal: during a periodontal examination, pockets 4 mm deep were found in the area of the molars of the lower jaw; near other teeth the depth of the pockets was no more than 3 mm. Radiographs revealed minimal generalized horizontal bone loss (<10%). The level of hygiene was assessed as satisfactory. Periodontal diagnosis according to the American Academy of Periodontology is type II periodontal disease.
Risk: low.
Prognosis: good.
Biomechanical: the patient had no clinical or radiological signs of carious lesions. Several restorations were found on the posterior teeth, as well as small areas of erosion. Erosion was present on the anterior teeth of the upper and lower jaws, most likely due to dentin defects resulting from inadequate functional load. Loss of anterior tooth structure due to increased wear significantly increased the risk factor of treatment and negatively impacted its future prognosis.
Risk: moderate.
Prognosis: satisfactory.
Functional: the patient had no complaints regarding the function of the temporomandibular joints. During stress tests, no joint pathologies accompanied by corresponding sounds were detected. However, the patient noted stiffness and discomfort in the masticatory muscles on both sides. Signs of severe tooth wear ranging from 4 mm to 5 mm were found on all anterior teeth of the upper and lower jaws from canine to canine. Minimal wear was noted in the posterior teeth. According to the medical history, the patient stated that tooth wear had been progressing over the past 5 years. These criteria, particularly severe isolated wear of the anterior teeth, are consistent with a diagnosis of limited masticatory excursion (Figure 3 and Figure 4).
Risk: moderate
Prognosis: unsatisfactory.
Photo 3. View of the upper jaw: restoration of the posterior group of teeth and wear of the anterior group of teeth.
Photo 4. View of the lower jaw: restoration of the posterior group of teeth and wear of the anterior group of teeth (similar to the upper jaw).
Maxillofacial: With a full smile or an “ee-ee” sound without the lips obstructing the visualization of the teeth, the patient had barely one-third of his front teeth visible. At rest, the teeth are not visible. With a wide smile, the patient’s gum level was also not visualized, which was due to low lip dynamics and the factor of minimal dental visualization.
Risk: low.
Prognosis: hopeless.
Treatment Goals
The goals of treatment formed a kind of triad.
- The first goal was to improve the aesthetic appearance of the smile through conservative, minimally invasive treatment.
- The next goal was to reduce functional risk and improve functional and maxillofacial prognosis while minimizing the need for tooth extraction and maximizing support for gingival health. This could be achieved through orthodontic repositioning of the teeth, which would help correct the condition of limited chewing ability and provide the necessary amount of space to restore the upper and lower anterior teeth to the more optimal crown length of 10 mm.
- The third goal was to restore the anterior teeth initially with composite resin as a trial for a period of 6 months after completion of orthodontic treatment. This approach is compatible with the patient's financial capabilities, and at the same time it would help determine whether the length of the teeth is acceptable and appropriate for the installation of ceramic crowns at the end of treatment.
Treatment plan
The treatment plan consisted of the following steps.
- A detailed description of the diagnosis, treatment goals, and rehabilitation plan was sent to the orthodontist prior to his scheduled consultation with this patient. Such communication contributes to an effective and productive consultation with the patient during an orthodontic appointment. After consultation with the patient, a meeting was scheduled between the treating dentist and the orthodontist to discuss in detail the treatment goals and the actual results that can be achieved through orthodontic intervention.
- After completion of orthodontic treatment, it was planned to obtain a diagnostic wax-up model of the anterior teeth using models installed in the Kois Dento-Facial Analyzer.
- Obtaining a rigid template from a diagnostic model to test the possibility of direct restoration of teeth with a composite.
- After completion of the test period, the Kois deprogrammer is planned to be used to confirm a healthy, stable and acceptable occlusion or to possibly correct the occlusion if necessary.
- Preparation and production of e.max (Ivoclar Vivadent) ceramic crowns for the anterior teeth as the final stage of treatment.
Treatment phases
Stage 1. Orthodontic treatment.
The patient wore fully fixed braces and ligatures for 13 months. Intrusion of the upper and lower incisors of approximately 1 mm and inclination of the upper incisors of approximately 2 mm were performed. The lower incisors were fixed back in a horizontal position as far as possible. During the process of orthodontic treatment, the patient reported an improvement in the condition of the masticatory muscles and the elimination of their discomfort, which was associated with the elimination of the friction factor of the anterior teeth and the expansion of chewing capabilities. At the end of orthodontic treatment, the patient had an anterior open bite in the incisor area and class I occlusion behind the canines. Because the orthodontist was concerned about the need to stabilize the position of the incisors before completing the restoration, he placed a lingual retainer in the mandible and a full cap retainer in the maxilla (Figures 5 and 6).
Photo 5. View of the maximum tubercular-fissure contact of antagonist teeth after orthodontic treatment: there is a place for restoration.
Photo 6. Smile after orthodontic treatment: there is a place for restoration.
Stage 2. Preliminary restorative treatment.
Models of teeth after orthodontic treatment were compared using a Kois dentofacial analyzer. A diagnostic wax-up was made in a dental laboratory to recreate the normal length of the anterior teeth, aesthetically harmonizing with the patient's facial shape. A solid template was formed on the wax and sectioned to visualize the facial surfaces of the upper teeth. The palatal part of the template with the attached incisal edge was used to restore the upper teeth with direct composite (TPH3, DENTSPLY). The space for restoration obtained through orthodontic treatment did not allow restoration of both the upper and lower teeth at the same time. In order to adequately lengthen the crowns and recreate the correct contour of the upper anterior teeth, all available available space was required. Taking into account the dynamics of the lower lip, it was possible to achieve an acceptable aesthetic result. The trial composite restorations were adjusted in such a way that when the patient bit the 200 µm articulation paper, no marks were found that would correspond to possible functional occlusal interference (Figure 7 and Figure 8).
Photo 7. View of the maximum cusp-fissure contact of antagonist teeth: trial composite restorations.
Photo 8. Smile with trial composite restorations.
Stage 3. Deprogramming.
Six months after placement of direct composite restorations, a Kois deprogrammer was used to test and determine optimal occlusal function. The 6-month period was chosen to provide sufficient time for the new occlusion to settle and stabilize. This stage, however, turned out to be unnecessary, since no chips or signs of wear were diagnosed in the area of the teeth restored with the composite, which indicates their acceptable functioning. In addition, when the patient completed a dental post-orthodontic assessment form (Kois Center), he responded negatively to all questions related to bite problems, jaws, and jaw function.
Stage 4. Recovery.
Once the stability of the new tooth position was confirmed and the patient approved of the appearance of his new smile, the decision was made to permanently restore the maxillary anterior teeth using e.max crowns. Because the composite restorations were used as a guide shape and guide for the final crowns, a very acceptable esthetic result was achieved at the end of treatment (Figures 9-12).
Photo 9. View of the maximum tubercular-fissure contact of antagonist teeth after installation of e-max crowns on teeth 6-11.
Photo 10. Patient’s smile after installation of e-max crowns.
Photo 11. View of the upper jaw with installed crowns.
Photo 12. Close-up view of the installed crowns.
Discussion and conclusions
The physician should be interested in finding motivating factors for the patient who seeks dental care. Over time, the level of risk may increase and the prognosis of treatment may worsen, although the patient is well informed about the potential consequences without treatment. In this case, the patient did not have the necessary motivation until he got married, after which he began to take the problems of wearing his teeth and an unattractive smile more seriously.
Comprehensive dental treatment is often an interdisciplinary procedure and involves the treating physician working with other dental specialists and technicians as needed. In this case, close communication between the orthodontist and the dental laboratory at specific stages of treatment helped achieve exceptional aesthetic results and stabilize an acceptable functional occlusion.
Posted by Chris Wilson, DMD
How can you tell if the enamel is wearing off?
First, the top layer of enamel is affected - the tissue becomes more faded, and the bottom of the erosive lesion looks hard and smooth. A person experiences discomfort while eating due to increased tooth sensitivity. When eating too hot, cold or sweet food.
Many people mistakenly assume that worn enamel is a cosmetic problem. However, if the tissue surface is not restored in time, the enamel will continue to deteriorate, the damage will affect the dentin, and then the tooth pulp.
How to restore worn enamel?
What to do if the enamel on your teeth is worn away? Firstly, don’t worry - in the vast majority of cases, the tissue can be restored. And, if you recognize weakening teeth at an early stage, you can restore them to their former strength even at home.
In later stages of enamel destruction, you must consult a dentist. The doctor can perform one of the restorative procedures:
- Fluoridation of enamel
helps increase the resistance of teeth to aggressive substances - fruit acids, soda, tobacco. This treatment procedure can be used at any stage of enamel wear. - Placing fillings
will help restore the thickness of the enamel and strengthen damaged areas of the tooth. - Installation of veneers.
The thinnest plates installed on the teeth strengthen the enamel, replace the outer layer of crowns, and also correct the shape and color of the row. - Remineralization
or application of substances with calcium, fluoride, and vitamins to the teeth. The composition is absorbed almost instantly, covers damage and gradually strengthens the enamel.
If you notice that the enamel on your teeth has worn away in the initial stages of the disease, you can use home remedies to strengthen it. We have formulated several recommendations, following which you can restore the damaged layer.
- Be careful with products containing fluoride.
If you live in areas with high levels of fluoride in the water, you should never use fluoride toothpaste. Remember, excess fluoride is just as harmful as a deficiency of this element. - Eat right.
Do not forget that teeth need calcium, phosphorus, as well as vitamins D, A, K, C. Remember, dairy products, eggs, and raw vegetables and fruits are also useful for enamel. But it is better to avoid lemonade, alcoholic drinks and cigarettes to maintain dental health. - Include solid foods in your daily diet.
Carrots, apples, celery will help clean your teeth from food debris and perfectly strengthen the enamel. - Take good care of
your mouth and visit your dentist twice a year. - Massage your gums regularly.
With improved blood circulation, beneficial substances penetrate tissues faster and saturate them with vitamins. - Use natural remedies to strengthen enamel.
Tea tree solutions and herbal decoctions have proven themselves to be excellent. For thinned enamel, even rinsing with sea salt is helpful. To prepare a saline solution, simply dissolve 4 teaspoons of salt in half a glass of water. - Remember about folk remedies.
Even in Soviet times, activated carbon, lemon zest, and baking soda served as faithful assistants in the fight for strong, healthy teeth.
A useful product for enamel is green tea. Just one glass of this refreshing drink a day will help reduce your chances of losing teeth by 15-20% and strengthen your enamel.
Dentists recognize ASEPTA PLUS toothpaste Remineralization as one of the most effective means of strengthening worn enamel. This product is designed to strengthen weakened enamel and protect gums from inflammation. The paste contains hydroxyapatite, a source of natural bioactive calcium and phosphorus, thermal mud, the enzyme papain, which breaks down plaque, zinc and potassium, as well as extracts of Eleutherococcus and calendula, which accelerate the regeneration processes of the oral mucosa (a special case during pregnancy).
When should you start taking care of your teeth?
The correct answer is from the prenatal period. It is from this time that the expectant mother should saturate her body with vitamins and calcium and take vitamin and mineral complexes specially created for pregnant women. A professional dentist will help in this matter.
Breastfeeding is important for a newborn baby, because mother's milk will provide the baby with everything necessary for proper development, including teeth.
When the child gets older, parents introduce him to sweets - this is the first factor that destroys teeth. From this moment on, there is a danger of caries. If there is not enough calcium, the enamel will be destroyed in childhood.
To avoid such danger, the mother must:
- Reduce consumption of sugar and fructose;
- Protect yourself from any diseases so as not to cause hypoplasia in the unborn child - underdevelopment of tooth enamel;
- Feed your baby breast milk, because the share of sugar in infant formula is up to 30%;
- Minimize the amount of cookies and sweets in the child’s diet;
- Take vitamins as prescribed by your dentist.