The term "tonsillitis" comes from the Latin name for the tonsils or tonsils. These are special paired rounded almond-shaped formations located on both sides between the palate and the root of the tongue, on the border of the oral cavity and pharynx. Their basis is lymphoid tissue; it is responsible for the maturation of lymphocytes (immunocompetent cells) and the development of an immune response with their help.
The palatine tonsils belong to the peripheral immune organs and, together with other tonsils, form the protective lymphopharyngeal ring of Pirogov-Waldeyer. Their task is to recognize and subsequently destroy pathogens and create an immune barrier at the level of the pharynx. Such protection works both against infectious agents penetrating from outside and against one’s own opportunistic flora.
In most cases, this process is asymptomatic. But sometimes it is not possible to quickly destroy the pathogens; they begin to multiply in the natural recesses (crypts and lacunae) of the tonsils and provoke inflammation. This condition is called tonsillitis.
There are 2 forms of the disease:
- Acute tonsillitis or tonsillitis, the duration of the disease usually does not exceed 10–14 days. The nature of the inflammation can be catarrhal, follicular or lacunar. After the pathogen is destroyed, all symptoms of the disease are leveled, and the tonsils are cleared and return to their previous state.
- Chronic tonsillitis, characterized by prolonged inflammation of the tonsils. The tonsils are enlarged, and a purulent-microbial (caseous) substrate is constantly preserved in their recesses.
Chronic form of tonsillitis, why the tonsils become inflamed
Infection is the main cause of inflammation of the tonsils. The acute form of the disease in 70% of cases is caused by viruses, the remaining 30% is caused by bacterial and fungal flora. Therefore, sore throats most often accompany acute respiratory infections and are seasonal.
Damage to the tonsils in chronic tonsillitis in 80% of cases is of a bacterial nature. The main causative agents of the disease:
- β-hemolytic streptococcus.
- Group A streptococcus.
- Staphylococcus aureus.
- Haemophilus influenzae.
- Rarely encountered bacteria: mycoplasma, chlamydia, etc.
Viruses in the chronic form of the disease have a predominantly provocative, destabilizing effect. Acute and chronic recurrent viral infections weaken the immune defense, which creates conditions for the activation of bacterial flora. Hypothermia, acute intoxication, and ingestion of cold or irritating food lead to the same result.
Chronic tonsillitis
Your child is undergoing surgery. We would like to give you and your child information about the need for this intervention. We make sure that you do not feel helpless in this situation. We would like to acquaint you with the essential aspects of the operation itself, and the risk factors in case of its failure. The written information provided to you serves this purpose. Read it carefully to discuss any unclear points with your doctor.
Every healthy child has lymphoid tissue in the pharynx, which is united into the so-called lymphadenoid pharyngeal ring. It includes the palatine tonsils - “tonsils” - they can be seen when examining the mouth - they look like balls protruding on the sides of the tongue, the pharyngeal tonsil - it cannot be seen during a direct examination of the oral cavity, it hides in the nasopharynx, behind the palate, lingual tonsil - located at the root of the tongue, and many lymphoid follicles scattered along the back wall of the pharynx, at the entrance to the larynx (see Fig. 18). These formations help the child defeat pathogenic bacteria that enter the throat during breathing and eating, and contribute to the formation of local immunity - protection against pathogens. By the way, in these organs there are no cells that affect the sexual development of the child, they do not produce sex hormones, therefore their diseases do not affect the sexual development of the child, and if they are removed if necessary (more on this later), sexual development is not disrupted.
In early childhood - usually from 2 to 5-7 years - the described organs work very hard, as the child expands the scope of contacts with peers by attending kindergarten, and inevitably often becomes infected and develops respiratory diseases. Moreover, if the child’s immune forces are not strong enough due to congenital characteristics, environmental factors and other reasons, the lymphoid organs increase in volume. This enlargement of the palatine tonsils is called “hypertrophy of the palatine tonsils”; they can become inflamed - inflammation of the tonsils is called tonsillitis. Tonsillitis can be acute or chronic. In children, chronic tonsillitis and adenoids - an enlarged pharyngeal tonsil - are often combined.
The tonsils of the pharynx have a significant impact on the state of health and the development of nearby organs. What kind of influence is this? A noticeable obstruction to the passage of air through the nose leads to breathing through the mouth. The consequence is obvious - untreated air enters the respiratory tract - not purified, not warmed and not humidified. A chronic inflammatory process, constantly smoldering in the tissue of the tonsils and adenoids, periodically exacerbating, contributes to protracted, recurrent diseases of the trachea and bronchi (bronchitis, obstructive bronchitis, tracheitis, pharyngitis), can independently cause or aggravate the course of allergies, in severe cases manifested in the form of bronchial asthma , allergic rhinopathy, atopic dermatitis. Adenoids and enlarged palatine tonsils, filling the pharynx, impair the functioning of the auditory tubes, which cannot supply sufficient air to the middle ear, as a result of which secretory otitis media develops, which can lead to hearing loss, and if infection enters the ear, to its acute inflammation – acute purulent otitis media. Poor breathing through the nose contributes to improper development of the maxillofacial area - the bite of the teeth is disrupted, the shape of the face changes (the so-called “adenoid face”).
The causative agents of infectious diseases of the respiratory tract (most often streptococci) after a sore throat remain in the palatine tonsils, and their chronic inflammation develops - chronic tonsillitis. Under unfavorable circumstances (hypothermia, stress, viral infection), the process in the tonsils is activated. This occurs in the form of another sore throat with plaque on the tonsils or purulent plugs. What is very dangerous is that each exacerbation of tonsillitis can cause complications in the form of diseases of other organs and systems of the child’s body, most often rheumatic diseases of the heart and joints, kidney diseases (pyelitis, pyelonephritis, glomerulonephritis). In addition, exacerbation of tonsillitis or tonsillitis sometimes causes complications in the form of an abscess (ulcer) in the pharynx. This complication is called peritonsillar abscess. A peritonsillar abscess indicates that the palatine tonsil is unable to cope with its function; it can recur at any time.
What factors contribute to enlargement of the pharyngeal tonsils and the development of chronic tonsillitis?
- Heredity - at least if the parents suffered from adenoids or tonsillitis, the child, to one degree or another, will also face this problem.
- Inflammatory diseases of the nose, throat, pharynx - and respiratory viral infections, and measles, and whooping cough, and scarlet fever, and tonsillitis, etc.
- Eating disorders - especially overfeeding.
- Tendency to allergic reactions, congenital and acquired immunity deficiency.
- Violations of the optimal properties of the air that the child breathes - very warm, very dry, a lot of dust, an admixture of harmful substances (ecological conditions, excess household chemicals).
- Inadequate (incorrect) treatment of acute tonsillitis (tonsillitis). The most common mistakes are an incomplete course of antibiotic treatment, incorrect dosing, violation of the therapeutic and protective regime (early getting out of bed, walking outside before 7-10 days from the start of treatment).
Thus, the actions of parents aimed at preventing chronic tonsillitis come down to correction, and even better, to the initial organization of a lifestyle that promotes the normal functioning of the immune system - feeding according to appetite, physical activity, hardening, limiting contact with dust and household chemicals.
What is the difference between chronic tonsillitis and tonsil hypertrophy?
Hypertrophy of the tonsils is an increase in their size in the age of a child up to 9-10 years. With chronic tonsillitis, the tonsils can be of any size; its distinctive feature is the development of a chronic inflammatory process in the tonsils.
What if a child, along with chronic tonsillitis or enlarged tonsils, has adenoids?
The presence of adenoids and difficulty in nasal breathing significantly influence the development of tonsil disease. In this case, otolaryngologists suggest that in the case of a compensated form of tonsillitis, while preserving the palatine tonsils, it is necessary to remove the adenoids, and in the case of a decompensated form, include adenotomy in the scope of the operation to remove the palatine tonsils, which slightly lengthens the operation and is almost imperceptible to the patient, but greatly affects the result of the operation. If this is not done, the child has a high probability of progression of tonsillitis or adenoiditis, which will negate the results of tonsillectomy - difficult nasal breathing will persist, the child will again become ill often, snoring will not go away or will worsen.
When is tonsillitis treated and when is surgery performed?
There are two forms of chronic tonsillitis: compensated and decompensated. In the decompensated form, surgical treatment is not possible - the tonsils must be removed. This diagnosis is made when tonsillitis often worsens (2-3 sore throats per year), the process extends beyond the tonsils, if diseases of distant organs and systems develop, for example, nephritis, rheumatic diseases of the heart and joints. Tonsils must be removed if a peritonsillar abscess develops.
Is it possible and necessary to treat chronic tonsillitis?
Let us emphasize that treatment is not only possible, but also necessary. Until the child develops the changes mentioned earlier, every six months, local treatment should be carried out in the form of irrigation of the pharyngeal mucosa with aqueous solutions that have anti-inflammatory, antiallergic and antimicrobial properties, as well as general treatment methods, including vitamin preparations, agents that affect immune system, locally acting vaccine preparations, physiotherapeutic methods (magnetic and laser therapy, inhalations). Otolaryngologists consider it particularly important in the treatment of tonsillitis to conduct a course of washing the lacunae of the palatine tonsils (7-10 procedures per course of treatment).
How urgently should the operation be performed?
The operation to remove the tonsils - tonsillectomy - is planned, that is, it is performed when the child is in full health or in remission of chronic diseases. It cannot be performed during acute illnesses (ARI) and 3-4 weeks after recovery. Thus, it is always possible to perform this operation in a period favorable for the child, which will minimize the risk of postoperative complications.
Do palatine tonsils grow again, are relapses possible?
No, completely removed tonsils cannot grow back.
How are tonsils removed?
This operation is performed using local or general anesthesia (narcosis). It lasts 25-30 minutes and, with proper psychological preparation of the child, is tolerated satisfactorily. The simplicity of the operation does not indicate its safety. Complications due to anesthesia, bleeding, and damage to the palate are also possible. But all this does not happen often.
Surgeons have long abandoned the removal of tonsils using ultrasound and laser due to the huge risk of complications.
How long does a child stay in the hospital after surgery?
Due to the high risk of bleeding in the postoperative period, the child is in the hospital for 6 days after surgery.
What should you do after your baby is discharged?
The child is discharged from the hospital under the supervision of an ENT doctor or pediatrician at the clinic at the place of residence. Home treatment is usually recommended for 1-2 weeks. In this case, physical activity should be limited, however, there is no need to keep the child in bed. When eating during the first days, you should not eat hot, spicy foods, sour juices and fruits, carbonated drinks, or ice cream. After 5-7 days, the diet becomes normal. 10-14 days after discharge, if the child’s general condition is satisfactory, there is no elevated body temperature, and the wound in the pharynx is healing smoothly, you can visit the children’s group and go outside. You can’t just do sports or go to the pool. The wound in the pharynx heals completely in 3-4 weeks. A month after the operation, there are no restrictions in lifestyle or diet.
How to remove tonsils at the Children's City ENT Center?
To establish a diagnosis, if there is no ENT doctor in the clinic, you can make an appointment at the city ENT consultation office by calling 2-78-49-00 (inquiry).
Reception is carried out on weekdays, from 8.00. until 20.00.
If the diagnosis of “chronic tonsillitis” has been established and you have made the decision to operate on your child, with a referral for surgical treatment issued at the clinic, you should go to the emergency department of the 3rd Children’s Clinical Hospital at any time convenient for you. Your child will be registered for hospitalization on the day you choose and will be given an examination plan (a list of tests necessary to perform the operation). Hospitalization is carried out on Tuesday and Thursday, from 13.00. until 15.00. and on Sunday from 16.00. until 18.00. The operation is carried out the next day.
Features of the chronic form of the disease
Chronic inflammation of the tonsils can have several clinical variants:
- Latent form, when the patient does not experience significant discomfort in the throat and does not experience signs of exacerbation of the disease. Such people consider themselves healthy and are not aware of the dormant infectious-inflammatory focus in their throat.
- Periodically relapsing type of disease. Sluggish exacerbations and episodes of clearly defined inflammation of the tonsil itself, adjacent palatine arches and the pharyngeal wall are possible. Between periods of exacerbation, the inflammatory process subsides, but is not completely eliminated.
In chronic tonsillitis, the drainage and natural self-cleaning of crypts (folds) and lacunae (recesses) are disrupted in the tonsils; pus, living and dead bacteria, and toxins are constantly stored in their depths. This maintains constant inflammation, overstimulates sentinel immune cells, and provokes toxic-allergic reactions.
The immune response that forms during chronic tonsillitis is not sufficient to completely suppress the infectious process; it only restrains the activity of pathogens. Disruption of this delicate balance leads to exacerbation of the disease or triggers immune disorders.
Features of the acute stage of the disease
Acute tonsillitis or tonsillitis is a rapidly developing and short-lived infectious inflammation of the tonsils, followed by complete regression of symptoms and a return of the lymphoid tissue of the pharynx to its original state. Often the inflammatory process involves the adjacent palatine arches and the mucous membrane of the pharynx, which is called tonsillopharyngitis.
Characteristic manifestations of angina include:
- Rapid onset of the disease, development of the main symptoms within a few hours.
- A sore throat. It intensifies with swallowing, and its localization depends on the side of the lesion.
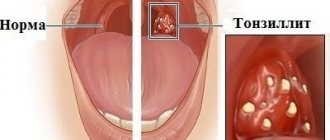
- Redness, swelling, enlargement of the tonsils and palatine arches. With the catarrhal form of the disease there are no other changes. With follicular angina, whitish-yellow lesions appear on the surface, as if translucent from the inside, and the lacunar form is characterized by the appearance of plaques and purulent films.
- Increased body temperature, signs of general intoxication.
- Enlargement and tenderness of the submandibular and upper cervical lymph nodes.
If the disease is treated incorrectly, the tonsils may remain enlarged and inflamed even after the patient’s well-being returns to normal. In their crypts, purulent plugs remain, and the protective function is disrupted. The tonsils themselves become a focus of infection, which can periodically activate and spread.
Why treat chronic tonsillitis?
Chronically inflamed tonsils become a constant source of infection. With a decrease in immunity, it can spread to other tonsils and peripharyngeal tissue, invade the nasal cavity and paranasal sinuses, and descend into the underlying parts of the respiratory tract.
But the inflammatory reaction of the tonsils is not the main problem of chronic tonsillitis. Constant irritation of the immune forces not only weakens the protective response, but also creates the preconditions for the occurrence of abnormal reactions. Antibodies appear in the body, which are initially produced against β-hemolytic streptococcus, but show aggression towards connective tissue.
This secondary pathology is called rheumatism or Sokolsky-Buyo disease. It is a systemic acquired disease with an autoimmune mechanism, with the favorite targets for antibodies being heart valves and the synovium of small joints.
The key focus of streptococcal infection and the site of primary formation of rheumatic autoantibodies is the inflamed tonsils. Therefore, competent treatment of chronic tonsillitis is an effective prevention of rheumatism and its complications.
How to be treated correctly
Competent treatment of chronic tonsillitis includes a set of measures to eliminate infectious inflammation and deep sanitation (cleansing) of the tonsils. This is necessary to prevent relapses of the disease, suppress allergic and autoimmune processes, and restore the protective function of the pharyngeal lymphadenoid ring.
Common mistakes when treating tonsils:
- Only local medicine for sore throat is used, with the rejection of recommended systemic antibacterial therapy.
- The drug is selected by the patient independently, without taking into account the nature of inflammation, composition and sensitivity of the microflora.
- Drugs for the treatment of chronic tonsillitis are taken haphazardly, or instead of recommended medications, a folk remedy for the disease is used.
- Early cessation of treatment, therapy is completed soon after the sore throat subsides and other symptoms of exacerbation decrease.
- Avoidance of treatment between periods of exacerbation, refusal of proposed surgery.
- Late visit to the doctor, at the stage of complications.
This approach is the main reason for the protracted and complicated course of the disease and the formation of drug resistance in pathogens. Treatment of chronic tonsillitis in adults should be carried out comprehensively, under the supervision of a physician.
Conservative methods of treatment. Are they effective?
Treatment of acute tonsillitis in children of different ages and adults is traditionally carried out conservatively. But such therapy has a number of disadvantages:
- Antiseptic local remedies for sore throat act superficially and do not last long, and are quickly washed off with saliva. Therefore, when using them, it is impossible to achieve complete cleansing of the tonsil crypts and cope with deep-seated foci of inflammation.
- Local treatment of acute tonsillitis in children is often associated with certain difficulties. Parents are faced with the insufficient effectiveness of rinses and the child’s negative attitude towards the use of sprays and inhalations.
- The use of antibiotics is associated with inhibition of the native microflora of the oral cavity, intestines, and genitals. The resulting dysbiosis (dysbiosis) negatively affects well-being and digestion, and disrupts the functioning of the immune system. Therefore, many parents prefer to treat their child’s disease without using antibiotics, increasing the risk of complications.
- Antimicrobial agents should be selected taking into account the sensitivity of the microflora isolated from the tonsils, and the bacteriological analysis necessary for this takes several days and is not always available.
- Patients often complete treatment immediately after the sore throat disappears, without following the recommended duration of antibiotic therapy. This is fraught with the preservation of a dormant infectious focus, creating conditions for relapse of the disease and the development of microflora resistance.
- In most cases, it is not possible to limit yourself to using only one drug, and complex therapy requires time and adherence to a specific treatment regimen.
To fully cure acute tonsillitis means not only to relieve the patient of intoxication and sore throat. A competent doctor tries to achieve complete sanitation (cleansing) of the tonsils and elimination of the inflammatory reaction, but conservative therapy cannot always provide an adequate solution to this problem.
Treatment without surgery
Conservative treatment includes general and local drug therapy, physiotherapy, lavage of lacunae and other methods of cleansing the tonsils. Antibacterial, anti-inflammatory, antiallergic, and immunomodulatory agents are prescribed.
Conservative therapy is widely used in modern otorhinolaryngology. But it does not always completely cure tonsillitis. The tonsils may remain enlarged even after drug suppression of the infection and deep cleansing; the risk of relapses and complications remains. In approximately 1/3 of patients, it becomes necessary to treat the disease surgically.
Operations for tonsillitis: from traditional methods to modern techniques
Indications for surgical treatment:
- The presence of episodes of exacerbation of the disease 2 or more times a year, with a predominance of purulent inflammation.
- Frequent (more than 4 times a year) exacerbations of tonsillitis, even if they occur without complications.
- Exacerbations are rare, but there are signs of complications from the heart, joints, kidneys or other organs.
- The disease is latent (hidden), but has become the cause of the development of rheumatism and other systemic diseases.
For a long time it was believed that chronically inflamed tonsils should be completely removed. This operation is called tonsillectomy. It allows you to eliminate the source of infection, but makes an uncorrectable hole in the protective lymphoid ring of the pharynx.
Currently, tonsillectomy is rarely performed, mainly in cases of severe purulent-destructive changes in the tonsils. In all other cases, ENT doctors give preference to organ-preserving operations, trying to leave an island of functionally active tonsil tissue.
But resection (partial cutting off of the tonsils) carries the risk of relapse of the disease. After all, such a procedure does not guarantee the elimination of all inflamed and infected tissue. The use of a laser improves the result due to an additional disinfecting and immunomodulating effect in the surgical area, but still does not completely solve the problem of relapses. Nevertheless, laser technologies are recognized as a priority in the treatment of tonsillitis.