Finlepsin® (Finlepsin®)
Monotherapy for epilepsy begins with a low initial dose, gradually increasing it until the desired therapeutic effect is achieved.
When selecting the optimal dose, it is advisable to determine the concentration of carbamazepine in the blood plasma, especially during combination therapy. In some cases, the optimal dose may deviate significantly from the recommended initial and maintenance dose, for example, due to the induction of microsomal liver enzymes or due to interactions during combination therapy.
Finlepsin® should not be combined with sedative-hypnotics. If necessary, it can be combined with other substances used to treat alcohol withdrawal. During treatment, it is necessary to regularly monitor the content of carbamazepine in the blood plasma. Due to the development of side effects from the central and autonomic nervous system, patients are closely monitored in a hospital setting. When transferring a patient to carbamazepine, the dose of the previously prescribed antiepileptic drug should be gradually reduced until it is completely discontinued. Sudden cessation of carbamazepine may trigger epileptic seizures. If it is necessary to abruptly interrupt treatment, the patient should be transferred to another antiepileptic drug under the cover of the drug indicated in such cases (for example, diazepam administered intravenously or rectally, or phenytoin administered intravenously).
Several cases of vomiting, diarrhea and/or decreased nutrition, convulsions and/or respiratory depression have been described in newborns whose mothers took carbamazepine concomitantly with other anticonvulsants (these reactions may represent neonatal withdrawal syndrome). Before prescribing carbamazepine and during treatment, liver function testing is necessary, especially in patients with a history of liver disease, as well as in elderly patients. If existing liver dysfunction worsens or active liver disease develops, the drug should be discontinued immediately. Before starting treatment, it is necessary to conduct a study of the blood picture (including counting platelets, reticulocytes), iron level in the blood serum, general urine analysis, urea level in the blood, electroencephalogram, determination of the concentration of electrolytes in the blood serum (and periodically during treatment, because hyponatremia may develop). Subsequently, these indicators should be monitored weekly during the first month of treatment and then monthly.
In most cases, a transient or persistent decrease in the number of platelets and/or leukocytes is not a precursor to the onset of aplastic anemia or agranulocytosis. However, before starting treatment, and periodically during treatment, clinical blood tests should be performed, including platelet counts and possibly reticulocyte counts, and serum iron levels should be determined. Non-progressive asymptomatic leukopenia does not require discontinuation, however, treatment should be discontinued if progressive leukopenia or leukopenia accompanied by clinical symptoms of an infectious disease occurs. Carbamazepine should be discontinued immediately if hypersensitivity reactions or symptoms suggestive of Stevens-Johnson syndrome or Lyell's syndrome occur. Mild skin reactions (isolated macular or maculopapular exanthema) usually disappear within a few days or weeks, even with continued treatment or after reducing the dose of the drug (the patient should be under close medical supervision at this time).
The possibility of activation of latent psychoses should be taken into account, and in elderly patients, the possibility of developing disorientation or psychomotor agitation.
In some cases, treatment with antiepileptic drugs was accompanied by the occurrence of suicide attempts/suicidal intentions. This was also confirmed in a meta-analysis of randomized clinical trials using antiepileptic drugs. Since the mechanism of suicide attempts when using antiepileptic drugs is not known, their occurrence cannot be ruled out when treating patients with Finlepsin®. Patients and staff should be warned to monitor for suicidal thoughts/behavior and to seek immediate medical attention if symptoms occur.
Male fertility and/or spermatogenesis disorders are possible, but the relationship between these disorders and carbamazepine has not yet been established.
Intermenstrual bleeding may occur with simultaneous use of oral contraceptives. Carbamazepine may adversely affect the reliability of oral contraceptives, so women of reproductive age should use alternative methods of birth control during treatment.
Carbamazepine should only be used under medical supervision. Patients should be informed of early signs of toxicity, as well as skin and liver symptoms. The patient is informed of the need to immediately consult a doctor in case of adverse reactions such as fever, sore throat, rash, ulceration of the oral mucosa, causeless bruising, hemorrhages in the form of petechiae or purpura.
Before starting treatment, it is recommended to conduct an ophthalmological examination, including fundus examination and measurement of intraocular pressure. If the drug is prescribed to patients with increased intraocular pressure, constant monitoring of this indicator is required.
Patients with severe cardiovascular diseases, liver and kidney damage, as well as elderly people are prescribed lower doses of the drug. Although the relationship between the dose of carbamazepine, its concentration and clinical efficacy or tolerability is very small, regular determination of carbamazepine levels may be useful in the following situations: with a sharp increase in the frequency of attacks; to check whether the patient is taking the drug properly; during pregnancy; when treating children or adolescents; if there is a suspicion of impaired absorption of the drug; if toxic reactions are suspected if the patient is taking several medications.
During treatment with Finlepsin® it is recommended to refrain from drinking alcohol.
Nosological classification (ICD-10)
- F10.3 Withdrawal state
- F25 Schizoaffective disorders
- F28 Other non-organic psychotic disorders
- G35 Multiple sclerosis
- G40 Epilepsy
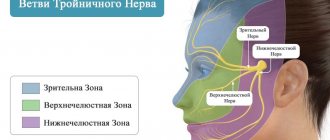
- G50.0 Trigeminal neuralgia
- G52.1 Lesions of the glossopharyngeal nerve
- G63.2 Diabetic polyneuropathy (E10-E14+ with common fourth character .4)
- R20.2 Paresthesia of the skin
- R25.2 Cramp and spasm
- R27.0 Ataxia, unspecified
- R47.1 Dysarthria and anarthria
- R52.9 Pain, unspecified
Limitations and adverse reactions
Contraindications to the use of the drug are:
- severe forms of depression - with them there is a high probability of suicidal thoughts and actions;
- phobias, obsessions - possible increase in aggression;
- allergic reactions;
- uncompensated respiratory failure.
The drug is prescribed with caution to elderly people due to their increased susceptibility to it. It is not recommended to use it at this age for too long a time.
The drug is contraindicated for children under 18 years of age. It can be taken only in rare cases after carefully weighing the need and risks. In this case, therapy should be short-term.
Taking the drug in the 1st trimester of pregnancy is contraindicated. It easily crosses the placental barrier and can cause developmental defects in the child. Grandaxin can pass into breast milk, so you should avoid breastfeeding while treating with the drug.
Otherwise, when it enters the child’s body, it accumulates and causes a sedative effect. The newborn's sucking reflex decreases, he cannot suck out milk fully, and loses weight.
Despite the mild effect of the drug, it still exhibits some side effects:
- headaches, agitation and aggressiveness;
- sleep problems;
- confusion;
- increased frequency of seizures in epileptic patients;
- breathing disorders;
- poor appetite, thirst, digestive problems;
- jaundice;
- muscle hypertonicity, muscle pain;
- allergic manifestations.
In such cases, taking the drug is canceled.
Indications for Finlepsin® retard
epilepsy: primary generalized seizures (with the exception of absence seizures), partial forms of epilepsy (simple and complex seizures), secondary generalized seizures;
trigeminal neuralgia;
idiopathic glossopharyngeal neuropathy;
pain due to damage to peripheral nerves in diabetes mellitus, pain due to diabetic neuropathy;
epileptiform convulsions in multiple sclerosis, spasms of the facial muscles in trigeminal neuralgia, tonic convulsions, paroxysmal speech and movement disorders (paroxysmal dysarthria and ataxia), paroxysmal paresthesia and attacks of pain;
alcohol withdrawal syndrome (anxiety, convulsions, hyperexcitability, sleep disturbances);
psychotic disorders (affective and schizoaffective disorders, psychoses, disorders of the limbic system).
Pharmacokinetics
Absorption is slow but complete (food intake does not significantly affect the speed and extent of absorption). After a single dose of the tablet, Cmax is reached after 32 hours. The average Cmax of unchanged active substance after a single dose of 400 mg of carbamazepine is about 2.5 μg/ml. Css of the drug in plasma are achieved in 1–2 weeks (the speed of achievement depends on the individual characteristics of metabolism: autoinduction of liver enzyme systems, heteroinduction by other simultaneously used drugs), as well as on the patient’s condition, the dose of the drug and the duration of treatment. There are significant individual differences in Css values in the therapeutic range: in most patients these values range from 4 to 12 μg/ml (17–50 μmol/l). Concentrations of carbamazepine-10,11-epoxide (a pharmacologically active metabolite) are approximately 30% of those of carbamazepine. Communication with plasma proteins in children is 55–59%, in adults – 70–80%. Apparent Vd - 0.8–1.9 l/kg. In the cerebrospinal fluid and saliva, concentrations are created that are proportional to the amount of active substance not bound to proteins (20–30%). Penetrates through the placental barrier. The concentration in breast milk is 25–60% of that in plasma. Metabolized in the liver, mainly along the epoxide pathway with the formation of the main metabolites - active carbamazepine-10,11-epoxide and an inactive conjugate with glucuronic acid. The main isoenzyme that ensures the biotransformation of carbamazepine into carbamazepine-10,11-epoxide is cytochrome P450 (CYPZA4). As a result of these metabolic reactions, a metabolite, 9-hydroxymethyl-10-carbamoylacridan, is also formed, which has weak pharmacological activity. Carbamazepine can induce its own metabolism. T1/2 after oral administration of a single dose is 60–100 hours (on average about 70 hours); with prolonged use, T1/2 decreases due to autoinduction of liver enzyme systems. After a single oral dose of carbamazepine, 72% of the dose taken is excreted in the urine and 28% in the feces; in this case, about 2% of the dose taken is excreted in the urine in the form of unchanged carbamazepine, about 1% - in the form of a 10,11-epoxide metabolite.
There is no data indicating that the pharmacokinetics of carbamazepine changes in elderly patients.
Drug therapy
Drug therapy involves the use of the following groups of drugs:
- Anticonvulsants (Lyrica, Neurontin, others). These drugs have shown good effectiveness against neuropathic pain. However, they have a number of side effects, the most common of which are decreased concentration, drowsiness and swelling of the legs;
- Antidepressants. Some antidepressants (Amitriptyline, Duloxetine) affect the production of special brain substances that are responsible for both depressive states and the perception of pain. Doctors often prescribe minimal doses of antidepressants in the complex treatment of postherpetic neuralgia. Their main side effects include: drowsiness, dry mouth, dizziness;
- In cases of severe pain and insufficient effectiveness of other drugs, patients may be prescribed narcotic analgesics.
Causes of postherpetic neuralgia
Once a person has had chickenpox, the virus remains in the body for life. With age, the immune system weakens (particularly from taking medications or chemotherapy) and the virus can become more active, resulting in shingles.
Damage to nerve endings during rashes leads to postherpetic neuralgia. When damaged, nerve fibers cannot send signals from the skin to the brain as they normally do. Instead, they transmit amplified signals, and the patient feels excruciating pain that can last for months or even years.
Overdose
Symptoms: symptoms that occur during overdose usually reflect disorders of the central nervous system, cardiovascular and respiratory systems.
Central nervous system and sensory organs: depression of central nervous system functions, disorientation, drowsiness, agitation, hallucinations, coma, blurred vision, slurred speech, dysarthria, nystagmus, ataxia, dyskinesia, hyperreflexia (initially), hyporeflexia (later), convulsions, psychomotor disorders, myoclonus, hypothermia, mydriasis.
Cardiovascular system: tachycardia, decreased blood pressure, sometimes increased blood pressure, intraventricular conduction disturbances with widening of the QRS complex, fainting, cardiac arrest.
Respiratory system: respiratory depression, pulmonary edema.
Digestive system: nausea and vomiting, delayed evacuation of food from the stomach, decreased colon motility.
Urinary system: urinary retention, oliguria or anuria, fluid retention, hyponatremia.
Laboratory indicators: leukocytosis or leukopenia, hyponatremia, possible metabolic acidosis, hyperglycemia and glycosuria, increased muscle fraction of creatine phosphokinase.
Treatment: there is no specific antidote. Symptomatic supportive treatment in the intensive care unit, monitoring of heart function, body temperature, corneal reflexes, kidney and bladder function, and correction of electrolyte disorders are necessary. It is necessary to determine the concentration of carbamazepine in plasma to confirm poisoning with this drug and assess the degree of overdose, gastric lavage, and the administration of activated charcoal. Late evacuation of gastric contents can lead to delayed absorption on days 2 and 3 and the reappearance of symptoms of intoxication during the recovery period). Forced diuresis, hemodialysis and peritoneal dialysis are ineffective, however, dialysis is indicated for a combination of severe poisoning and renal failure. Children may require blood transfusions.
Compound
| Long-acting tablets | 1 table |
| active substance: | |
| carbamazepine | 200 mg |
| 400 mg | |
| excipients: Eudragit® RS30D (ethyl acrylate, methyl methacrylate and trimethylammonioethyl methacrylate copolymer (1:2:0.1) - 11/22 mg; triacetin - 2.2/4.4 mg; talc - 15.6/31.2 mg; Eudragit® L30D-55 (methacrylic acid and ethyl acrylate copolymer) - 35/70 mg; MCC - 21.8/43.6 mg; crospovidone - 12.4/24.8 mg; colloidal silicon dioxide - 1.33/2, 66 mg; magnesium stearate - 0.67/1.34 mg |
How to recognize depression
As already mentioned, the drug helps get rid of depression, but not all of its forms. Grandaxin is taken only for mild to moderate disease with moderately severe symptoms.
During the course of the disease, several syndromes are distinguished:
- Emotional disorders: low mood, melancholy, anxiety and internal tension, pessimistic attitude; self-flagellation, lack of interest in the world around us, inability to have fun.
- Behavioral reactions: solitude, reduced activity; bad habits;
- Cognitive functions: inability to concentrate, slow thinking, decreased memory and perception; pessimistic thoughts, thoughts of suicide, low self-esteem.
- Autonomic disorders: poor sleep, appetite distortion, weakness and malaise, intestinal dysfunction; discomfort in the heart and other organs, headaches.
A specific indication for the use of the drug is reactive depression. It develops in response to the action of some traumatic factor. The condition is characterized by a consistently reduced emotional background and fixation on the problem.
The patient reproaches and blames himself for what happened, his conversations are aimed only at the problem. And, constantly analyzing it, he seeks support from those around him.
A person is worried about insomnia. And he is fully aware of his condition.
Attacks of despair and demonstrative hysterics are possible. Excitement reaches a state called “melancholic raptus.” At the same time, the person rushes about aimlessly, sobs, screams, and suicide attempts are not ruled out.
This state can be replaced by a depressive stupor, when the patient “freezes” in one position, not reacting to what is happening.