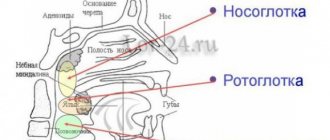
Anatomy of the human upper and lower jaws. Their structure and functions.
The jaws are part of the human facial skeleton. The upper and lower jaws are not connected to each other at the skeletal level and are connected only by soft tissues.
Schoolchildren often make the mistake of claiming that the upper and lower jaw are united by a joint. But in reality, the lower jaw is connected by a joint to the temporal bone , and this joint is called the temporomandibular joint .
Jaw structure: temporomandibular joint
The human lower jaw is the only movable bone in the human skull. And the joint that provides this mobility is special; it provides movement in three directions at once: vertical movements (opening and closing the mouth), horizontal movements (moving the lower jaw from side to side), and pushing the lower jaw forward.
The human upper jaw , anatomically speaking, is much larger in the area where the upper teeth grow. The upper jaw ends only in the area of the bridge of the nose, where it is fixedly connected to the frontal bone. It turns out that the bones of the face that surround the nose up to the bridge of the nose and the inner corners of the eyes are all the upper jaw. Scientifically speaking, the upper jaw has four processes: the alveolar (where the teeth grow), the frontal, the zygomatic and the palatine, which forms our hard palate.
Human skull bones, upper jaw highlighted in pink
The human upper jaw is considered an air-bearing bone, since it contains the maxillary sinuses , anatomically these are cavities in the bone lined with epithelium. This epithelium is ciliated, that is, it ensures the movement of air inside the sinus; it also contains glands that secrete mucus.
It is interesting that scientists are still not completely clear why a person needs the maxillary sinuses; some say that they are needed to warm and humidify the air, others hypothesize that they house a whole internal laboratory of the body, where it studies microbes that enter them from the environment.
Maxillary sinus or sinus
The structure of the human jaw: teeth and their formula
When citing one number for any tooth, the dentist means its anatomical and functional affiliation. If you conditionally divide the dentition into two halves and start counting from the first incisor, you will get 8 teeth in each direction (top and bottom). The first incisor is a one. The second, accordingly, is a deuce. And so on until the last molar, which is called the figure eight. If the doctor says - bottom seven on the left, then we are talking about the bottom left second molar. As you can see, everything is very simple!
This can be expressed schematically as follows (permanent teeth):
For baby teeth, everything is the same, only the teeth are designated by Roman numerals (there are no premolars in the primary dentition):
As for the two-digit designations, they were invented in order to simplify the written recording of medical history. The above is preserved, but a number appears before the number indicating which jaw and on which side the tooth is located. Conventionally, the oral cavity is divided into segments - upper right (number 1), upper left (number 2), lower left (number 3), lower right (number 4). As you noticed, the report is conducted starting from the top right and clockwise. The segment is written first, and then the tooth number. For example, the third canine from the top right would be designated tooth 13. The lower incisor on the left is 32 teeth. In children, the segments are designated by numbers 5 to 8, so as not to confuse the primary bite with the permanent one. Let's take the same third fang on the right. In a child, it will be designated as tooth 53. And so on by analogy. The main thing is to always start the report from the right side at the top, then you won’t get confused. These are not snails with 25 thousand teeth! Can you imagine their dental formulas?
Useful information for patients
The jaws are the basis of the facial skeleton. Not only the beauty of the profile depends on their anatomical structure, but also functional capabilities that are important for life - chewing, swallowing, breathing, speech, the formation of cavities for the sensory organs and much more.
SYMPTOMS OF CORRECT BITE:
- There are no gaps between teeth.
- Chewing is not difficult.
- There is clear pronunciation.
- There are no cracks, chips or stains on the enamel.
- The teeth have the correct shape.
- There is no crowding of teeth.
- There is no pronounced inclination of the teeth in or out.
- The center of the incisors is located right in the middle of the face.
With improper development of bone tissue and the alveolar process, deformations such as microgenia, prognathia, overbite and others occur. In adults, the shape can also change, and this is mainly due to factors such as:
- Severe mechanical injuries.
- Consequence of surgical interventions.
- Various pathological processes (osteomyelitis, ankylosis, purulent inflammation and others).
- Incorrect orthodontic treatment or relapses after it.
- Partial or complete adentia (senile jaw).
Changes in structure, various inflammatory and tumor processes lead to severe diseases of the jaw. The most common pathologies are osteitis, periostitis, osteomyelitis. At the first signs, such as swelling, redness, pain, fever, you should contact a dentist or surgeon.
ANATOMY OF THE JAW
UPPER JAW
The upper jaw is a fixed paired bone of the facial skeleton. It has an air cavity (sinus), 4 surfaces (orbital, anterior, posterior, internal), as well as 4 processes (frontal, zygomatic, palatine and alveolar).
The dentition of the upper jaw is deviated slightly forward and outward. The crowns of the teeth increase in size from the incisor to the first molar, but the second molar is smaller than the first, the third is smaller than the second. The height of the crowns decreases successively from the incisor to the third molar, with the exception of the canines. The large roots of the teeth provide significant stability to the dentition of the upper jaw and to each tooth individually.
LOWER JAW
The lower jaw is a movable horseshoe-shaped bone of the facial skeleton. A large number of muscles are attached to it. The dentition of the lower jaw has a parabolic shape.
The teeth of the lower jaw are characterized by the fact that the incisors and canines are located perpendicular to the alveolar process, the chewing teeth are slightly inclined towards the tongue. The pattern of changes in the size and height of tooth crowns on the lower jaw is the same as on the upper jaw.
JAW DEVELOPMENT
The growth and formation of the jaw is closely related to the development of tooth germs and alveolar process. This process begins as early as the 7th week of intrauterine life. It is influenced by various endogenous factors (maternal toxicosis, hormonal imbalances, levels of vitamins and minerals), and after the birth of a child - also exogenous (external).
The jaw of a newborn is not yet completely ossified and fused; the lower part is shifted back in relation to the upper.
When a permanent dentition is formed (from the age of 6), intensive growth occurs due to the eruption of molars and incisors. Also, growth spurts are observed at 11–13 years of age; in boys, this usually occurs later. By the age of 18, the formation of bone tissue is completely completed.
CHANGES IN THE SHAPE OF THE LOWER JAW WITH AGE
| Jaw of a newborn |
| Jaw of a 4 year old child |
| Jaw of a 6 year old child |
| Jaw of an adult |
| Elderly man's jaw |
For patients who want to get a free consultation with a dentist in Krasnodar , we inform you that pre-registration for an appointment is being made at Dentistry on Gagarin. Call the numbers indicated on the website and sign up for a free consultation with a dentist with a diagnosis (consultation duration up to 15 minutes).
Anatomical structure of the tooth
We figured out the order of the teeth. Further - more interesting! After all, a tooth is a unique organ, designed by nature to perform very important functions, primarily chewing. To be firmly held in the jaw bone, you need a root. The longest root is at the canine. Teeth can be single-rooted or multi-rooted. The structure of the upper teeth (molars) is somewhat more complex than that of the lower ones, since they have 3 roots. There are especially many variations in the number and type of roots in “wisdom teeth.” But the visible part of the tooth protruding above the gum is called the crown. It has different shapes in the incisors, canines and molars to perform the functions of biting, crushing or chewing food. The boundary between the crown and the root is the neck of the tooth. It is usually not visible, but it can become exposed due to certain diseases (periodontal disease, etc.). An x-ray is a kind of photo of the structure of the tooth and will give you an idea of what the state of affairs is in the oral cavity.
Facial bones
The upper jaw (maxilla) (Fig. 59) is paired and participates in the formation of the orbit, oral and nasal cavities, infratemporal and pterygopalatine fossae. Coming together, both upper jaws, together with the nasal bones, limit the opening leading to the nasal cavity and called the pyriform aperture. In the temporal bone itself there is a body and four processes.
In the thickness of the body of the upper jaw (corpus maxillae) there is an air-bearing maxillary, or maxillary, sinus (sinus maxillae), which communicates with the nasal cavity. There are four surfaces in the body. The orbital surface (facies orbitalis) (Fig. 76) is smooth, triangular in shape, directed upward and takes part in the formation of the lower wall of the orbit.
The infraorbital groove (sulcus infraorbitalis) runs along the orbital surface (Fig. 76), continuing into the infraorbital canal (canalis infraorbitalis). The canal contains vessels and nerves; it opens on the anterior surface with the infraorbital foramen (foramen infraorbitale) (Fig. 76). The orbital surface is separated from the anterior surface by a sharp infraorbital edge (margo infraorbitalis) (Fig. 76). On the anterior surface (facies anterior) there are the canine, or canine, fossa (fossa canina) (Fig. 76) and the infraorbital foramen (foramen infraorbitale) (Fig. 76). On the nasal surface (facies nasalis), which participates in the formation of the lateral wall of the nasal cavity, there is a cleft of the maxillary sinus (hiatus maxillaris) (Fig. 77). Anterior to the cleft, the tear groove (sulcus lacrimalis) runs from top to bottom (Fig. 76, 77). The infratemporal surface (facies infratemporalis) (Fig. 77) is convex, contains alveolar openings (foramina alveolaria) (Fig. 76), through which blood vessels and nerves are directed to the teeth. In the lower part of the infratemporal surface there is the maxillary tubercle (tuber maxillae) (Fig. 76).
| Rice. 76. Upper jaw external view 1 - frontal process; 2 - tear groove; 3 - orbital surface; 4 - infraorbital groove; 5 - infraorbital margin; 6 - maxillary tubercle; 7 - infraorbital foramen; 8 - zygomatic process; 9 - alveolar openings; 10 - canine fossa; 11 - alveolar elevations |
The frontal process (processus frontalis) (Fig. 76, 77) rises vertically upward and connects with the nasal part of the frontal bone. The zygomatic process (processus zigomaticus) (Fig. 76, 78) is massive, directed sideways and connects with the zygomatic bone. The alveolar process (processus alveolaris) (Fig. 77) goes down and has an arched shape. On its free lower edge there are 8 dental alveoli (alveoli dentales) (Fig. 78), which are separated from each other by interalveolar septa (septa interalveolaria) (Fig. 78), and on the outer surface, in accordance with the location of the teeth, there are alveolar elevations (juga interalveolaria) (Fig. 76).
| Rice. 77. Upper jaw, inside view 1 - frontal process; 2 - tear groove; 3 - cleft of the maxillary sinus; 4 - infratemporal surface; 5 - palatine process; 6 - alveolar process |
The palatine process (processus palatinum) (Fig. 77, 78) is located horizontally and, connecting with the process of the same name on the opposite side using the median palatine suture (sutura palatina mediana) (Fig. 78), forms the anterior large part of the hard palate.
| Rice. 78. Upper jaw ventral view 1 - dental alveoli; 2 - palatine process; 3 - zygomatic process; 4 - median palatal suture; 5 - interalveolar septa |
The lower jaw (mandibula) (Fig. 59) is connected to the temporal bone with a joint, and therefore has great mobility. It has a body and two branches.
The body of the lower jaw (corpus mandibulae) (Fig. 79, 81) has the shape of an arcuate plate. The upper edge of the body of the lower jaw is called the alveolar part (pars alveolaris) (Fig. 79) and is limited by the alveolar arch (arcus alveolaris), containing the dental alveoli for 16 teeth. The lower edge is called the base of the lower jaw (basis mandibulae) (Fig. 79), it is quite massive, rounded, with thickened compact bone substance. On its convex outer surface there is a chin protuberance (protuberantia mentalis) (Fig. 79, 81), lateral to which, at the level of small molars, there is a mental foramen (foramen mentale) (Fig. 79, 81) which is the exit of the mandibular canal (canalis mandibulae). The inner surface is concave, with the mental spine (spina mentalis) protruding in the middle (Fig. 80), under which is located the digastric fossa (fossa digastrica) (Fig. 80) - the place of attachment of the digastric muscle, and laterally there is the location of the sublingual salivary gland - the hypoglossal fossa (fovea sublingualis). Here, the maxillary-hyoid line (linea mylohyoidea) (Fig. 80) runs diagonally, posteriorly and downward from which there is a gentle depression - the location of the submandibular salivary gland - the submandibular fossa (fovea submandibularis) (Fig. 80). The mylohyoid groove (sulcus mylohyoideus) is also located here (Fig. 80), which is a trace of the vessels and nerve.
| Rice. 79. Lower jaw external view 1 - condylar process; 2 - coronoid process; 3 - notch of the lower jaw; 4 - opening of the lower jaw; 5 - tongue of the lower jaw; 6 - branch of the lower jaw; 7 - chewing tuberosity; 8 - alveolar part; 9 - body of the lower jaw; 10 - chin hole; 11 - angle of the lower jaw; 12 - chin protuberance; 13 - base of the lower jaw | |
| Rice. 80. Lower jaw, inside view 1 - tongue of the lower jaw; 2 - opening of the lower jaw; 3 - mylohyoid groove; 4 - mental spine; 5 - maxillary-hyoid line; 6 - digastric fossa; 7 - submandibular fossa; 8 - pterygoid tuberosity; 9 - angle of the lower jaw |
Each branch of the lower jaw (r. mandibulae) (Fig. 79) rises from the posterior end of the body, heading almost vertically upward. The place where the branch leaves the body is called the angle of the lower jaw (angulus mandibulae) (Fig. 79, 80). The upper ends of the branches bifurcate, forming the notch of the lower jaw (incisura mandibulae) (Fig. 79).
In front of the notch there is a sharp coronoid process (processus corocoideus) (Fig. 79, 81), and behind it there is a condylar process (processus condylaris) (Fig. 79, 81). In the area of the angle of the lower jaw, on the outer surface there is a masticatory tuberosity (tuberositas masseterica) (Fig. 79), and on the inner surface there is a pterygoid tuberosity (tuberositas pterygoidea) (Fig. 80). Both are places of attachment for muscles of the same name. Under the notch on the inner surface of the branch there is an opening of the lower jaw (foramen mandibulae) (Fig. 79, 80), which represents the beginning of the canal of the lower jaw. In front, the opening is limited by the tongue of the lower jaw (lingual mandibulae) (Fig. 79, 80, 81). The canal lies deep in the branches and body of the lower jaw, has an arched shape and contains blood vessels and nerves for the teeth. As mentioned above, it ends on the outer surface of the body with the mental opening.
| Rice. 81. Lower jaw, top view 1 - condylar process; 2 - tongue of the lower jaw; 3 - coronoid process; 4 - interalveolar septa; 5 - body of the lower jaw; 6 - chin hole; 7 - chin protuberance |
| Rice. 82. Palatine bone A - external view; B — internal view: 1 — orbital process; 2 - sphenoid process; 3 - sphenopalatine notch; 4 - perpendicular plate; 5 - horizontal plate |
| Rice. 83. Zygomatic bone A - external view; B - view from the inside. |
| Rice. 84. Hyoid bone 1 - greater horn; 2 - small horn; 3 - body of the hyoid bone |
The palatine bone (os palatinum) is paired. Both parts are connected to each other by means of a horizontal plate (lamina horizontalis) (Fig. 82), thus forming the posterior sections of the bony palate. The lateral wall of the nasal cavity is formed by a perpendicular plate (lamina perpendicularis) (Fig. 82), which consists of the anterior orbital process (processus orbitalis) (Fig. 82) and the posterior sphenoid process (processus sphenoidalis) (Fig. 82). The processes are separated from each other by the sphenopalatine notch (incisura sphenopalatina) (Fig. 82).
The zygomatic bone (os zygomaticum) (Fig. 59, 83) connects with the zygomatic processes of the upper jaw, frontal and temporal bones, thereby taking part in the formation of the orbit, temporal fossa and zygomatic arch.
| Rice. 85. Lacrimal bone A - external view; B - view from the inside. |
| Rice. 86. Nasal bone A - external view; B - view from the inside. |
The hyoid bone (os hyoideum) (Fig. 84) has the shape of a horseshoe and is located under the lower jaw, lying deep in the muscles of the neck. It contains the body of the hyoid bone (corpus ossis hyoidei) (Fig. 84), a pair of small horns (cornua minora) (Fig. 84) going to the top, and a pair of large horns (cornua majora) (Fig. 84) going to back.
| Rice. 87. Inferior turbinate A - external view; B — inside view: 1 — lacrimal process; 2 - ethmoid process; 3 - maxillary process |
The lacrimal bone (os lacrimale) (Fig. 59, 85) is a thin flat plate of a quadrangular shape and forms the anterior section of the medial wall of the orbit. Together with the frontal process of the maxilla, it takes part in the formation of the fossa of the lacrimal sac.
The nasal bone (os nasale) (Fig. 59, 86), connecting with the bone of the same name on the opposite side, forms the back of the nose.
The inferior nasal concha (concha nasalis inferior) (Fig. 87) is a thin long plate bent along the axis. It contains the maxillary process (processus maxillaris) (Fig. 87), the lacrimal process (processus lacrimalis) (Fig. 87) and the ethmoidal process (processus ethmoidalis) (Fig. 87). One of its edges is attached to the lateral wall of the nasal cavity, the other hangs freely into the nasal cavity, separating the middle and lower nasal passages.
| Rice. 88. Vomer A - side view; B - top view. |
The vomer (Fig. 88) is a thin quadrangular plate. Together with the perpendicular plate of the ethmoid bone, it takes part in the formation of the bony septum of the nasal cavity.
The temporomandibular joint (articulatio temporomandibularis) is a pair, formed by the articulation of the mandibular fossa and the articular tubercle of the temporal bone with the articular surface of the condylar process of the mandible. The capsule is attached along the edge of the articular surfaces using the lateral ligament (lig. laterale), which runs from the zygomatic process of the temporal bone to the neck of the condylar process of the mandible. The articular disc (discus articularis) fuses with the capsule, which is located in the joint cavity, dividing it into upper and lower sections. The shape of the joint is condylar, movement occurs simultaneously in both joints.
The lowering and raising of the lower jaw is carried out around the frontal axis. Between the articular disc and the head of the lower jaw, minor movements are possible, for example during speech. When the mouth is opened strongly, the head of the lower jaw and the articular disc come out onto the articular tubercle of the temporal bone. The extension of the lower jaw is carried out due to the sliding of the head of the lower jaw and the articular disc along the articular fossa and the articular tubercle of the temporal bone. The displacement of the lower jaw to the side is ensured by rotation around the vertical axis of the head of the lower jaw of the side in which the movement is made, and by the extension of the head of the lower jaw of the opposite side together with the articular cartilage.
Histological structure of the tooth
The special hardness of teeth is due to their structure. The outside of the crown is covered with enamel, the basis of which is hydroxyapatite crystals. 96% of the enamel consists of inorganic substances, which is why it is so hard (which, however, does not mean that experiments can be carried out on teeth, testing their strength). But dentin, which is located under the enamel, has much less inorganic substances - about 70%. It is softer, and therefore is destroyed by caries more than enamel. Inside the tooth there is a cavity filled with a neurovascular bundle, or pulp. The entire rich spectrum of pain during the deepening of the carious process is associated with it. In addition to nerve fibers, the pulp also contains a large number of blood vessels, through which infection from the affected tooth spreads throughout the body. This is why it is so dangerous to leave dental diseases untreated.
Structure of the lower jaw
A - top view : 1 - head of the lower jaw; 2 - pterygoid fossa; 3 - coronoid process; 4 - mandibular pocket; 5 - molars; 6 - body of the lower jaw; 7 - premolars; 8 - fang; 9 - incisors; 10 - mental tubercle; 11 - chin protuberance; 12 - interalveolar septa; 13 - dental alveoli; 14 - chin hole; 15 - interroot septa; 16 - angle of the lower jaw; 17 - outer wall of the alveoli; 18 - oblique line; 19 — inner wall of the alveoli; 20 - retromolar fossa; 21 - buccal ridge; 22 — notch of the lower jaw; 23 - tongue of the lower jaw; 24 - neck of the lower jaw. ; B - rear view : 1 - incisors; 2 - fang; 3 - premolars; 4 - molars; 5 - coronoid process; 6 - condylar process; 7 - tongue of the lower jaw; 8 - mylohyoid groove; 9 - mylohyoid line; 10 - submandibular fossa; 11 - pterygoid tuberosity; 12 - digastric fossa; 13 - mental spine; 14 - sublingual fossa; 15 - angle of the lower jaw; 16 - canal of the lower jaw; 17 - neck of the lower jaw.
The structure of the lower jaw . B — internal view : 1 — buccal ridge; 2 - temporal crest; 3 - notch of the lower jaw; 4 - head of the lower jaw; 5 - neck of the lower jaw; 6 - tongue of the lower jaw; 7 - opening of the lower jaw; 8 - mylohyoid groove; 9 - mandibular ridge; 10 - pterygoid tuberosity; 11 - mylohyoid line; 12 - angle of the lower jaw; 13 - submandibular fossa; 14 - sublingual fossa; 15 - digastric fossa; 16 - compact substance of the lower jaw; 17 - spongy substance of the lower jaw; 18 — incisors; 19 - fang; 20 - premolars; 21 - molars
In the middle of the outer surface of the jaw body there is a chin protuberance (protuberantia mentalis), which is a characteristic feature of modern humans and determines the formation of the chin. The angle of the chin relative to the horizontal plane in modern humans ranges from 46 to 85°. On both sides of the mental protuberance, closer to the base of the jaw, there are mental tubercles (tubercula mentalia). Outside of them is the mental foramen (foramen mentale), which is the outlet of the mandibular canal. The vessels and nerves of the same name exit through the mental foramen. Most often, this hole is located at the level of the 5th tooth, but it can move anteriorly to the 4th tooth, and posteriorly to the space between the 5th and 6th teeth. The dimensions of the mental foramen range from 1.5 to 5 mm, its shape is oval or round, sometimes it is double. The mental foramen is removed from the base of the jaw by 10-19 mm; on toothless jaws of adults with an atrophied alveolar part, it is closer to the upper edge of the jaw.
In the lateral parts of the body of the lower jaw there is an obliquely located ridge - an oblique line (linea obliqua), the anterior end of which corresponds to the level of the 5-6th tooth, and the rear end, without sharp boundaries, passes to the anterior edge of the ramus of the lower jaw. On the inner surface of the jaw body , near the midline, there is a bone spine, sometimes double, called the mental spine (spina mentalis). This place is the beginning of the geniohyoid and genioglossus muscles. Below and lateral to the mental spine is the digastric fossa (fossa digastrica), in which the digastric muscle begins. Above the digastric fossa there is a flat depression - the sublingual fossa (fovea sublingualis) - a trace from the adjacent sublingual salivary gland. Further posteriorly, the mylohyoid line (linea mylohyoidea) is visible, on which the superior pharyngeal constrictor and mylohyoid muscle begin. The maxillary-hyoid line runs between the digastric and sublingual fossae at the level of the 5-6th tooth and ends on the inner surface of the jaw branch. Under the maxillary-hyoid line at the level of the 5-7th tooth there is a submandibular fossa (fovea submandibularis) - a trace from the submandibular salivary gland located in this place. The alveolar part of the jaw body contains 8 dental alveoli on each side. The alveoli are separated from each other by interalveolar septa (septa interalveolaria). The walls of the alveoli facing the lips and cheeks are called vestibular, and the walls facing the tongue are called lingual. On the surface of the body, the alveoli correspond to alveolar elevations (juga alveolaria), which are especially well expressed at the level of the canine and 1st premolar. Between the alveoli of the incisors and the mental protuberance there is a subincisal depression (impressio subincisiva). The shape, depth and width of the alveoli, the thickness of their walls are different for teeth of different groups. The alveoli of the incisors (especially the central ones) are compressed from the sides, their bottom is shifted to the vestibular compact plate, therefore the thickness of the lingual wall of the alveoli is greater than the vestibular one. The alveoli of the canine and especially the premolars are rounded, the lingual wall is thicker than the vestibular one. The deepest alveoli of the canine and 2nd premolar. The thickness of their walls is greater than the alveoli of the incisors. The alveoli of molars are distinguished by the presence of interradicular septa. In the alveoli of the first two molars there is one septum separating the anterior and posterior chambers for the corresponding roots. The alveolus of the 3rd molar is varied in shape and number of septa, which is associated with the variability of the shape of this tooth. Most often the alveolus is conical, without septa, but may have one and sometimes two septa. The walls of the alveoli of the molars are thickened due to the oblique and mylohyoid lines. This strengthens the lower molars and protects them from loosening in the buccolingual direction during transversal lateral chewing movements.
The area located behind the 3rd molar is triangular in shape and is called the posterior molar fossa (fovea retromolaris). Laterally from this fossa, on the outer plate of the alveolar part, there is a mandibular pocket (recessus mandibulae), which stretches from the 2-3rd molar to the coronoid process (Fig. 1-13).
Rice. 1-13. The structure of the lower jaw, the outer surface (diagram according to V.P. Vorobyov ), part of the dense bone substance of the outer plate has been removed: 1 - condylar process; 2 - coronoid process; 3 - opening of the lower jaw; 4 - tongue of the lower jaw; 5 - buccal ridge; 6 - retromolar fossa; 7 - incisors; 8 - alveolar elevations; 9 - chin eminence; 10 - fang; 11 - premolars; 12 — roots of teeth; 13 - canal of the lower jaw; 14 - angle of the lower jaw; 15 - chewing tuberosity; 16 — notch of the lower jaw; 17 — tongue of the lower jaw (external view); 18 - molars
The structure of the alveoli of the lower jaw is similar to the structure of the alveoli of the upper jaw. The wall of the upper third consists of two layers: solid and compact plates (inner and outer). In the area of the bottom and lower third of the alveoli, under the hard plate there is a spongy substance. In the spongy substance of the body of the lower jaw there is a canal of the lower jaw (canalis mandibulae), through which vessels and nerves pass. The canal begins with the opening of the lower jaw (foramen mandibulae), on the inner surface of the branch and ends with the mental opening on the outer surface of the body. The canal has an arcuate direction with a convexity facing down and forward, lies closest to the bottom of the alveoli of the 2-3rd molar and passes between the chambers for their roots. Small tubules extend from the canal, through which vessels and nerves pass to the roots of the teeth; they open at the bottom of the alveoli. Medially from the mental foramen, the mandibular canal continues in the form of a small tubule to the midline and along this length gives off lateral branches to the bottom of the alveoli of the anterior teeth.
The branch of the lower jaw (ramus mandibulae) has outer and inner surfaces, anterior and posterior edges, which pass into the coronoid process (processus coronoideus) and the condylar process (processus condylaris), respectively. These processes are separated by the notch of the lower jaw (incisura mandibulae). The coronoid process serves to attach the temporal muscle, and the condylar process serves to form the temporomandibular joint (TMJ). The shape of the mandibular ramus varies individually (Fig. 1-14).
Rice. 1-14. Extreme forms of the basal arch of the lower jaw , ventral view: A - wide and short; B - narrow and long
The condylar process has a head (caput mandibulae) with an articular surface for connection with the mandibular fossa of the temporal bone and a neck (collum mandibulae). On the anteromedial surface of the neck of the condylar process there is a pterygoid fossa (fovea pterygoidea) - the attachment site of the external pterygoid muscle. The head of the articular process is flattened and occupies a position in which the axes drawn through the largest size of both heads intersect at the foramen magnum at an angle of 120-178°, open anteriorly. The shape and position of the head are individually different and depend on the operating conditions of the TMJ and the condition of its components. Deviations leading to changes in the volume and direction of movement in the joint change the shape and position of the articular heads. The anterior edge of the ramus of the lower jaw laterally passes into an oblique line on the outer surface of the jaw body, and medially reaches the posterior alveoli, thus limiting the retromolar fossa. The medial part of the ridge, formed at the site of the transition of the anterior edge into the walls of the posterior alveoli, stands out under the name of the buccal crest (crista buccinatoria), from which the buccal muscle begins.
The posterior edge of the branch passes into the base of the jaw, forming an angle (angulus mandibulae), the value of which ranges from 110 to 145° (usually 122-133°) and changes throughout life. In newborns it is close to 150°, decreases in adults with preserved teeth and maximum chewing load, and increases again in old people with complete loss of teeth (Fig. 1-15). The outer surface of the branch contains a masticatory tuberosity (tuberositas masseterica), which occupies most of the branch and the angle of the jaw and is the site of attachment of the masticatory muscle. On the inner surface of the branch in the area of the angle and adjacent sections there is a pterygoid tuberosity (tuberositas pterygoidea) - the place of attachment of the medial pterygoid muscle. On the same surface, in the middle, there is an opening for the lower jaw (foramen mandibulae), which is covered in front and above by an inconsistently pronounced bony protrusion - the tongue (lingula mandibulae). Above and anterior to the uvula is the mandibular ridge (torus mandibularis) - the place of attachment of two ligaments: the maxillary-pterygoid and the maxillary-sphenoid. The branches of the lower jaw are usually turned outward, so that the distance between the condylar processes of the right and left branches is greater than the distance between the outer points of the angles of the jaw. Can be distinguished as extreme forms of the jaw with maximally and minimally deployed branches. The degree of divergence of the branches depends on the shape of the upper half of the face. With a wide upper half of the face, the branches of the lower jaw are less developed than with a narrow upper half of the face. The smallest width of the branch, which usually falls in the middle of its height, ranges from 23 to 40 mm (usually 29-34 mm). The width and depth of the jaw notch are also individually different: the width of the notch is from 26 to 43 mm (usually 32-37 mm), the depth is from 7 to 21 mm (usually 12-16 mm). People with a wide upper half of the face usually have jaws with the greatest width of the notch and vice versa.
The structure of baby teeth
A temporary bite differs from a permanent bite not only in the number of teeth (in a temporary bite there are 20). Baby teeth have a bluish tint to the crown, which is also much wider than the root. Children have less enamel mineralization, so caries affects them very quickly, and the pulp takes up more space compared to permanent teeth. The canals of baby teeth are wider, easier to pass for instrumentation, and the roots themselves have a rounded shape. The structural features of baby teeth determine their rapid destruction in case of infection penetration and very severe pain in the child, so in childhood, visit the dentist in a timely manner.
Knowing the structure of teeth will help you quickly find a common language with the dentist and feel more confident when discussing treatment issues.
You will be able to better navigate the manipulations performed by the doctor and clarify all the points that interest you with an understanding of the essence of what is happening. This article is for informational purposes only, please consult your doctor for details!
Blood circulation and sensitivity in human jaws
In the human lower jaw there is a maxillary canal, an elongated narrow cavity through which the mandibular artery, vein and mandibular nerve pass. The upper jaw also has a maxillary artery, vein and nerve, but their structure, as can be seen from the figure below, is more branched.
These vessels and nerves provide nutrition and sensitivity to the teeth, but not only to them, they are also responsible for the sensitivity of the soft tissues of the face and partially provide blood circulation to them.
Blood circulation in the upper and lower jaw, as well as the facial nerve
If you look closely at the drawing, it becomes clear why half of the jaw, and sometimes even half of the face, can hurt because of one bad tooth. All these areas are united by the trigeminal nerve .
Nature has made sure that the facial nerve is reliably protected by bone tissue. But damage to it is dangerous because it can lead to loss of sensitivity and immobility of part of the face.
Structure of the lower jaw
Through the mental foramen , a bundle of nerves and blood vessels exits the body of the jaw into the soft tissues. Typically, the mental foramen is located between the 4th and 5th teeth, but its location may vary slightly from person to person.
About the blood circulation in the human jaws, we can say that the upper and lower jaw arteries are branches of the carotid artery. And venous blood from the jaws subsequently ends up in the jugular vein.
Blood supply to human jaws
Functions of the human upper and lower jaw
- Support function. The upper and lower jaw of a person serve as a support for the facial and chewing muscles. And there are many of these muscles; according to some reference books, a person has 57 separate muscles on the face alone.
- Protective function . The jaw bones protect the sensory organs and the upper digestive system.
- Digestion. Jaws are needed to bite and chew food. In addition, some muscles necessary for sucking and swallowing movements are attached to them.
- Breathing . The jaws serve as a container and support for the upper respiratory tract, in which air is filtered, humidified and heated.
- Speech. The jaws are involved in the process of articulation. Regulation of the opening of the mouth by the temporomandibular joint, the presence of teeth, the work of the muscles attached to the jaws - all this is necessary to make our speech intelligible.
- Facial expressions and communication. A movable lower jaw and facial muscles are necessary to reproduce emotions that are understandable to other people and communicate with the outside world.
INTERESTING: The mouth is the most developed part of the baby's body. This is where the most sensitive nerve endings are located, and therefore small children, in order to explore an object, pull it into their mouth.