An otolaryngologist (ENT) is a doctor who treats diseases of the ear, nose and throat (larynx, trachea, pharynx). To eliminate the risk of complications and progression of ENT diseases into chronic forms, it is important to consult a doctor in a timely manner. At the Istok Health Clinic you can visit a qualified otolaryngologist without referrals or certificates at any time convenient for you.
cost of services
Otolaryngology
| Otolaryngology | |
| Initial appointment with an ENT doctor | 1800 rub. |
| Repeated appointment with an ENT doctor | 1500 rub. |
| Initial appointment with an ENT doctor (candidate of medical sciences) | 2100 rub. |
| Repeated appointment with an ENT doctor (candidate of medical sciences) | 1800 rub. |
| Prof. inspection | 600 rub. |
| General ENT procedures | |
| Applying an ointment bandage to the skin or mucous membrane (one area) | 600 rub. |
| Applying a compress to the ear, behind the ear, or to the side of the neck (one anatomical area) | 600 rub. |
| Washing the postoperative cavity with solutions (single rinse) | 600 rub. |
| Application anesthesia (one anatomical area) | 290 rub. |
| Infiltration anesthesia (local, injection, one injection) | 340 rub. |
| Removal (removal) of sutures after ENT operations | 290 rub. |
| Local ENT manipulations and procedures: pharynx | |
| Irrigation of the posterior pharyngeal wall using an ENT combine | 170 rub. |
| Rinsing the lacunae of the palatine tonsils with a syringe (one tonsil) | 600 rub. |
| Vacuum lavage of the palatine tonsils using the TONZILLOR device | 1150 rub. |
| Removal of a foreign body from the oropharynx | 1150 rub. |
| Lubricating the back wall of the pharynx and palatine tonsils with medicinal solutions | 170 rub. |
| Opening a paratonsillar abscess | 2850 rub. |
| Separating the wound edges after opening the peritonsillar abscess | 1150 rub. |
| Ultrasonic irrigation session of the posterior pharyngeal wall and palatine tonsils (using the “TONSILOR” device) | 600 rub. |
| Shading of the follicles of the posterior pharyngeal wall with a solution of silver nitrate | 290 rub. |
| Removal of pharyngeal papilloma | 1150 rub. |
| Local ENT manipulations and procedures: larynx | |
| Removal of a foreign body from the hypopharynx | 1700 rub. |
| Infusion into the larynx from a syringe | 340 rub. |
| Changing the tracheotomy tube and aseptic dressing | 290 rub. |
| Medicinal irrigation of the larynx using an ENT combine | 170 rub. |
Anatomical structure of the pharynx
The pharynx, another name is the pharynx.
It starts at the back of the mouth and continues down the neck. The wider part is located at the base of the skull for strength. The narrow lower part connects to the larynx. The outer part of the pharynx continues with the outer part of the mouth - it has quite a lot of glands that produce mucus and help moisten the throat during speech or eating. When studying the anatomy of the pharynx, it is important to determine its type, structure, functions and risks of disease. As mentioned earlier, the pharynx is shaped like a cone. The narrowed part merges with the laryngopharynx, and the wide side continues the oral cavity. There are glands that produce mucus and help moisten the throat during communication and eating. From the front side it connects to the larynx, from above it adjoins the nasal cavity, on the sides it adjoins the cavities of the middle ear through the Eustachian canal, and from below it connects with the esophagus.
The larynx is located as follows:
- opposite 4 - 6 cervical vertebrae;
- behind - the laryngeal part of the pharynx;
- in front - formed due to the group of hyoid muscles;
- above - hyoid bone;
- lateral - adjacent to the thyroid gland with its lateral parts.
The structure of a child's pharynx has its own differences. Tonsils in newborns are underdeveloped and do not function at all. Their full development is achieved by two years.
The larynx includes in its structure a skeleton, which contains paired and unpaired cartilages connected by joints, ligaments and muscles:
- unpaired consist of: cricoid, epiglottis, thyroid.
- paired ones consist of: corniculate, arytenoid, wedge-shaped.
The muscles of the larynx are divided into three groups and consist of:
- thyroarytenoid, cricoarytenoid, oblique arytenoid and transverse muscles - those that narrow the glottis;
- posterior cricoarytenoid muscle - is paired and expands the glottis;
- vocal and cricothyroid - strain the vocal cords.
Entrance to the larynx:
- behind the entrance there are arytenoid cartilages, which consist of cornuform tubercles, and are located on the side of the mucous membrane;
- in front - epiglottis;
- on the sides there are aryepiglottic folds, which consist of wedge-shaped tubercles.
The laryngeal cavity is also divided into 3 parts:
- The vestibule tends to stretch from the vestibular folds to the epiglottis.
- Interventricular section - stretches from the inferior ligaments to the superior ligaments of the vestibule.
- Subglottic region - located at the bottom of the glottis, when it expands, the trachea begins.
The larynx has 3 membranes:
- mucous membrane - consists of multinucleated prismatic epithelium;
- fibrocartilaginous membrane - consists of elastic and hyaline cartilages;
- connective tissue - connects part of the larynx and other formations of the neck.
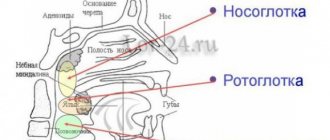
Pharynx: nasopharynx, oropharynx, swallowing department
The anatomy of the pharynx is divided into several sections.
- How is swallowing done?
Each of them has its own specific purpose:
- The nasopharynx is the most important section, which covers and merges with special openings into the back of the nasal cavity. The function of the nasopharynx is to moisturize, warm, clean the inhaled air from pathogenic microflora and recognize odor. The nasopharynx is an integral part of the respiratory tract.
- The oropharynx includes the tonsils and uvula. They border the palate and the hyoid bone and are connected by the tongue. The main function of the oropharynx is to protect the body from infections. It is the tonsils that prevent the penetration of germs and viruses inside. The oropharynx performs a combined action. Without its participation, the functioning of the respiratory and digestive systems is not possible.
- Swallowing department (hyopharynx). The function of the swallowing department is to carry out swallowing movements. The laryngopharynx is related to the digestive system.
There are two types of muscles surrounding the pharynx:
- stylopharyngeal;
- muscles are compressors.
Their functional action is based on pushing food towards the esophagus. The swallowing reflex occurs automatically when muscles tense and relax.
The process looks like this:
- In the oral cavity, food is moistened with saliva and crushed. The resulting lump moves towards the root of the tongue.
- Further, the receptors, irritating them, cause muscle contraction. As a result, the sky rises. At this second, a curtain closes between the pharynx and nasopharynx, which prevents food from entering the nasal passages. The lump of food moves deep into the throat without any problems.
- Chewed food is pushed down the throat.
- Food passes to the esophagus.
Since the pharynx is an integral part of the respiratory and digestive system, it is able to regulate the functions assigned to it. It prevents food from entering the respiratory tract during swallowing.
What functions does the pharynx perform?
The structure of the pharynx makes it possible to carry out serious processes necessary for human existence.
Functions of the pharynx:
- Voice-forming. Cartilage in the pharynx takes control of the movement of the vocal cords. The space between the ligaments is constantly subject to change. This process regulates the volume of the voice. The shorter the vocal cords, the higher the pitch of the sound produced.
- Protective. The tonsils produce immunoglobulin, which prevents a person from becoming infected with viral and antibacterial diseases. At the moment of inhalation, the air entering through the nasopharynx is warmed and cleared of pathogens.
- Respiratory. The air inhaled by a person penetrates the nasopharynx, then the larynx, pharynx, and trachea. The villi located on the surface of the epithelium prevent foreign bodies from entering the respiratory tract.
- Esophageal. The function ensures the functioning of swallowing and sucking reflexes.
The diagram of the pharynx can be seen in the next photo.
- The structure of the human throat and larynx: photo
Diseases affecting the throat and pharynx
Diseases of the ENT organs can be triggered by an attack of a viral or bacterial infection. But pathology is also caused by fungal infections, the development of various tumors, and allergies.
Pharynx diseases manifest themselves:
- ARVI;
- sore throat;
- tonsillitis;
- pharyngitis;
- laryngitis;
- paratonsillitis.
Only a doctor can determine an accurate diagnosis after a thorough examination and based on the results of laboratory tests.
Possible injuries
The pharynx can be injured as a result of internal, external, closed, open, penetrating, blind and through injuries. Possible complication - blood loss, suffocation, development of a retropharyngeal abscess, etc.
First aid:
- in case of injury to the mucous membrane in the oropharynx area, the damaged area is treated with silver nitrate;
- deep injury requires the administration of tetanus toxoid, analgesic, antibiotic;
- severe arterial bleeding is stopped by finger pressure.
Specialized medical care includes tracheostomy and pharyngeal tamponade.
The first is the voice, the second is the melody
A person’s ability to produce sounds of different strength, pitch and timbre is associated with the movement of the vocal cords under the influence of a stream of exhaled air. The strength of the sound produced depends on the width of the glottis: the wider it is, the louder the sound. The width of the glottis is regulated by at least five muscles of the larynx. Of course, the force of exhalation itself, caused by the work of the corresponding muscles of the chest and abdomen, also plays a role. The pitch of the sound is determined by the number of vibrations of the vocal cords in 1 second. The more frequent the vibrations, the higher the sound, and vice versa. As you know, tightly stretched ligaments vibrate more often (remember a guitar string). The muscles of the larynx, in particular the vocal muscle, provide the necessary tension to the vocal cords. Its fibers are woven into the vocal cord along its entire length and can contract either as a whole or in separate parts. Contraction of the vocal muscles causes the vocal cords to relax, causing the pitch of the sound they produce to decrease.
Having the ability to vibrate not only as a whole, but also in individual parts, the vocal cords produce additional sounds to the main tone, the so-called overtones. It is the combination of overtones that characterizes the timbre of the human voice, the individual characteristics of which also depend on the condition of the pharynx, oral cavity and nose, movements of the lips, tongue, and lower jaw. The airways located above the glottis act as resonators. Therefore, when their condition changes (for example, when the mucous membrane of the nasal cavity and paranasal sinuses swells during a runny nose), the timbre of the voice also changes.
Despite the similarities in the structure of the larynx of humans and apes, the latter are not able to speak. Only gibbons are capable of producing sounds that are vaguely reminiscent of musical sounds. Only a person can consciously regulate the force of exhaled air, the width of the glottis and the tension of the vocal cords, which is necessary for singing and speech. The medical science that studies the voice is called phoniatry.
Even in the time of Hippocrates, it was known that the human voice is produced by the larynx, but only 20 centuries later Vesalius (16th century) expressed the opinion that sound is produced by the vocal cords. Even now, there are various theories of voice formation, based on individual aspects of the regulation of vocal cord vibrations. Two theories can be cited as extreme forms.
According to the first (aerodynamic) theory, voice formation is the result of vibrational movements of the vocal folds in the vertical direction under the influence of an air stream during exhalation. The decisive role here belongs to the muscles involved in the exhalation phase and the muscles of the larynx, which bring the vocal cords together and resist the pressure of the air stream. Adjustment of muscle function occurs reflexively when the mucous membrane of the larynx is irritated by air.
According to another theory, the movements of the vocal folds do not occur passively under the influence of an air stream, but are active movements of the vocal muscles, carried out by command from the brain, which is transmitted along the corresponding nerves. The pitch of the sound, associated with the frequency of vibration of the vocal cords, thus depends on the ability of the nerves to conduct motor impulses.
Some theories cannot fully explain such a complex process as voice formation. In a person who has speech, the function of voice formation is associated with the activity of the cerebral cortex, as well as lower levels of regulation, and is a very complex, consciously coordinated motor act.
Anatomy of cartilage
When studying the structure of the larynx, special attention should be paid to the cartilage present.
They are presented as:
- Cricoid cartilage. This is a wide plate in the form of a ring, covering the back, front and sides. On the sides and edges, the cartilage has articular areas for connection with the thyroid and arytenoid cartilages.
- Thyroid cartilage, consisting of 2 plates that fuse in front at an angle. When studying the structure of a child’s larynx, these plates can be seen to converge in a rounded manner. This happens in women too, but in men it usually develops an angular protrusion.
- Arytenoid cartilages. They have the shape of pyramids, at the base of which there are 2 processes. The first, the anterior one, is the place for fastening the vocal cord, and the second, the lateral cartilage, is where the muscles are attached.
- Horn-shaped cartilages, which are located on the tops of the arytenoids.
- Epiglottic cartilage. It has a leaf-shaped form. The convex - concave surface is lined with mucous membrane, and it faces the larynx. The lower part of the cartilage extends into the laryngeal cavity. The front side faces the tongue.
Patients and methods
In 2016-2017 on the basis of City Clinical Hospital No. 1 named after. N.I. Pirogov, we observed 14 patients with PSG of various etiologies (9 women and 5 men) aged from 25 to 59 years. The cause of the development of PSG in 4 patients was long-term intubation, in 6 - GV and in 4 - idiopathic laryngeal stenosis. 5 patients had a tracheostomy at the time of admission to the hospital. All patients underwent clinical and laboratory examination, computed tomography of the larynx and trachea, endofibrolaryngotracheoscopy, examination of external respiration function, and consultations with related specialists.
According to endoscopic examination, all patients had a roller-like thickening of the mucous membrane of the subglottic part of the larynx; the mucous membrane was smooth, pink, and moist. No pathological discharge was detected in the trachea and main bronchi. According to the results of multislice computed tomography with three-dimensional reconstruction of the cartilaginous skeleton, in all patients at the level of the cricoid cartilage, a circular narrowing of the lumen was determined due to thickening and compaction of the soft tissues in the lumen. The length of the stenosis was 5–10 mm, the lumen diameter of its narrowest part was 4–9 mm. Three-dimensional reconstruction revealed no changes in the cartilaginous framework of the larynx, and its frame function was not impaired.
The operation was performed under anesthesia with the installation of direct support laryngoscopy and the use of video endoscopic technology. In 5 cases, intubation was performed through an existing tracheostomy. In 7 cases, the endotracheal tube was inserted beyond the level of the stenosis through the installed laryngoscope; in 2 patients it was installed above the stenosis. For intubation, tubes with an internal diameter of 5 and 6 mm were used.
Dilatation of cicatricial stenosis of the subglottic region of the larynx was performed when the oxygen content in the blood reached 100%. A balloon catheter was inserted into the lumen of the stenosis after the previously removed endotracheal tube. Using a special syringe-pressure gauge, liquid was pumped into a cylinder with a diameter of 10 mm, reaching a pressure of 10 atm. (exposure time 1 min), then the liquid from the balloon was evacuated and the balloon was removed. After reaching 100% saturation after 5-6 minutes, the procedure was repeated. Dilatation was carried out in three approaches, with artificial ventilation of the lungs performed between approaches.
It should be noted that in patients with severe scar changes in the tissues of the subglottic part of the larynx, lumen dilatation was performed after endoscopic dissection of the scar tissue using an electrosurgical scalpel.
To histologically confirm changes in the tissues of the subglottic part of the larynx during balloon dilation immediately before and after it, a biopsy of the subglottic part of the larynx was performed in 5 patients.
What is the throat, larynx and pharynx
A common misconception is to call the throat only the small area behind the tongue that turns red and hurts with sore throats. In this case, what is located below is often excluded. For example, there is a difference between the throat and larynx because it is part of this system below and is connected to the pharynx and trachea.
- Sore throat and fever, weakness in the body - what could it be? What to drink for these symptoms
The throat is not an anatomy term; it is the common name for the part of the upper respiratory tract from the hyoid bone to the level of the clavicle or manubrium of the sternum. The throat contains:
- pharynx or oropharynx - begins in the visible part of the mouth, the entrance gates are the tonsils, they are also tonsils that do not allow infections below;
- nasopharynx - cavities located above the palate;
- swallowing department - a small area behind the epiglottis that pushes food and liquids into the esophagus;
- The larynx is a cartilaginous tube for air, lined with mucous membrane and blood vessels.
Important to know: How to treat laryngeal paresis? We understand the aspects of the disease.
The epiglottis serves as a valve that prevents food and water from entering the larynx, at the top of which are the vocal folds (cords). Their closing and opening gives us the opportunity to make sounds. The larynx is protected in front by the thyroid cartilage, and behind it is the esophagus.
Functions of the larynx
It is customary to distinguish four main functions of the larynx: respiratory, protective, phonatory (voice-forming) and speech.
- Respiratory. When you inhale, air from the nasal cavity enters the pharynx, from it into the larynx, then into the trachea, bronchi and lungs. When you exhale, air from the lungs travels all the way through the respiratory tract in the opposite direction.
- Protective. The movements of the cilia covering the mucous membrane of the larynx continuously clean it, removing the smallest particles of dust that enter the respiratory tract. Dust surrounded by mucus is released as phlegm. Reflex cough is an important protective device of the larynx.
- Lamp room. The occurrence of sound is associated with vibration of the vocal cords during exhalation. The sound may vary depending on the tension of the ligaments and the width of the glottis. A person consciously regulates this process.
- Speech. It should be emphasized that only the formation of sound occurs in the larynx; articulate speech occurs when the organs of the oral cavity work: the tongue, lips, teeth, facial and masticatory muscles.
Possible diseases
Diseases of the nasal cavity are divided into four categories.
Allergic. Symptoms of such diseases manifest themselves through redness and sore throat, lacrimation, itching, and nasal discharge.
Inflammatory. With such diseases of the nasopharynx, general intoxication of the body is most often observed:
- chills,
- apathy,
- febrility,
- appetite and sleep disturbances.
And with tonsillitis - an increase in the size of the nasopharyngeal tonsils.
Traumatic. This category includes diseases characterized by bleeding, bone crepitus, sharp pain, redness and swelling of the affected area.
Oncological. Symptoms characteristic of this group of diseases include the presence of a malignant neoplasm, difficulty swallowing or breathing, a decrease in body weight by 7–10 kg over a month, general weakness of the body, an increase in the size of lymphatic formations, persistent low-grade fever for more than half a month.
Most of the causes of nasopharyngeal diseases can be corrected with medication or by leading a healthy lifestyle. However, a predisposing factor in the occurrence of oncological and allergic pathologies of this organ is burdened heredity, which in no way can be neutralized.
More dangerous pathologies
Any diseases of the nasopharynx are under the supervision of an otolaryngologist. The most common and dangerous pathologies are:
- Sore throat and complications caused by it (inflammation of the tonsils).
- Abscess is a purulent inflammation of the tonsils (a complication of tonsillitis).
- Pharyngitis is an inflammation of the mucous membrane of the pharynx.
- Adenoid vegetation - an increase in the size of the nasopharyngeal tonsils. With this pathology, breathing through the nose is completely impaired.
- Laryngitis is an acute inflammation of the mucous membrane of the larynx.
You can protect yourself from diseases of this organ by taking the following preventive measures:
- Rational and proper nutrition.
- Consumption of mineral and vitamin complexes.
- A healthy lifestyle is partly sports and physical exercise.
- Daily ventilation of living spaces.
Anatomical structure of the larynx
The larynx (larynx) is lined with various tissue structures, blood and lymphatic vessels, and nerves. The mucous membrane, covered from the inside, consists of multilayered epithelium. And underneath there is connective tissue, which in case of illness manifests itself as swelling. When studying the structure of the throat and larynx, we observe a large number of glands. They are absent only in the region of the edges of the vocal folds.
See the photo below for the structure of the human throat with a description.
The larynx is located in the throat in the shape of an hourglass. The structure of the larynx in a child differs from that of an adult. In infancy, she is two vertebrae higher than normal. If in adults the plates of the thyroid cartilage are connected at an acute angle, then in children they are at a right angle. The structure of the larynx in a child is also distinguished by a long glottis. In them it is shorter, and the vocal folds are of unequal size. The diagram of a child’s larynx can be seen in the photo below.
What does the larynx consist of?
The structure of the larynx in relation to other organs:
- superiorly, the larynx is attached to the hyoid bone by thyroid ligaments. This provides support for the external muscles;
- below, the larynx is attached to the first ring of the trachea with the help of the cricoid cartilage;
- on the side it borders on the thyroid gland, and on the back on the esophagus.
The skeleton of the larynx includes five main cartilages that fit tightly together:
- cricoid;
- thyroid;
- epiglottis;
- arytenoid cartilages - 2 pieces.
From above the larynx passes into the laryngopharynx, from below into the trachea. All cartilages found in the larynx, except the epiglottis, are hyaline, and the muscles are striated. They have the property of reflex contraction.
What functions does the larynx perform?
The functions of the larynx are determined by three actions:
- Protective. It does not allow third-party objects into the lungs.
- Respiratory. The structure of the larynx helps regulate air flow.
- Voice. The vibrations caused by the air are created by the voice.
The larynx is one of the important organs. If its functional activity is disrupted, irreversible consequences may occur.
Pain in the larynx
General information
The larynx is the upper part of the respiratory tract and also the organ of voice production. It is located at the level of the III-VI cervical vertebrae (slightly higher in children), opens from above into the pharynx, and below passes into the trachea. The skeleton of the larynx is formed by cartilages:
unpaired (cricoid, thyroid, epiglottis);
paired (arytenoid, corniculate, wedge-shaped)
They are connected to each other by joints and ligaments. The hypoglossoid membrane connects the larynx to the hyoid bone. Between the thyroid and cricoid cartilages is the cricothyroid ligament. It is sometimes resorted to dissection in case of acute laryngostenosis.
On the inner surface of the larynx there are vocal folds, the basis of which are paired vocal cords and vocal muscles. Above them are the vestibular folds, their basis is made up of the ligaments of the vestibule. Between the vestibular and vocal folds on each side are the ventricles of the larynx .
The space between the vocal folds is called the glottis. There are three sections in the laryngeal cavity: the upper, or vestibule (above the vestibular folds), the lower (under the vocal folds) and the middle, narrowest, located between the vestibular and vocal folds. The mucous membrane of the larynx is covered with columnar ciliated epithelium. On the vocal folds and upper parts of the epiglottis, the epithelium is multilayered squamous. The submucosal layer of the lower part of the larynx is loose, prone to swelling, especially in childhood. The larynx performs a respiratory, protective (spasm of the larynx and cough when a foreign body enters it or the presence of harmful impurities in the air) and voice-forming functions.
Pain in the larynx due to illness
With bruises, compression, cartilage fractures , or separation of the larynx from the trachea, shock may occur. Other signs of damage are expressed by the following characteristic symptoms:
- hemoptysis;
- pain in the larynx when swallowing and coughing;
- labored breathing.
On palpation , crepitus of the subcutaneous tissue (subcutaneous emphysema) and crunching of broken cartilages are noted. The victim may be at risk of suffocation caused by displacement, laryngeal edema and mediastinal emphysema. Poisoning with acids and caustic alkalis (acetic essence, soldering liquid, bath washing liquid, carbolic, oxalic acid, caustic soda, ammonia). Signs of poisoning are burns of the lips, oral mucosa, as well as:
- pain in the larynx;
- copious amounts of saliva;
- bloody vomiting.
The most common inflammatory diseases of the larynx are acute and chronic laryngitis. Less commonly, abscess, phlegmon, chondroperichondritis, diphtheria, tuberculosis and syphilis of the larynx develop. An abscess occurs as a result of the introduction of infectious agents during injury to the mucous membrane of the larynx. The disease initially occurs as a common sore throat, followed by hoarseness and difficulty breathing. Phlegmon of the larynx occurs with the following symptoms:
- high body temperature;
- chills;
- difficulty breathing;
- sharp pain in the larynx when swallowing,
Against this background, and also as a complication of influenza , chondroperichondritis of the larynx can occur, in which the inflammatory process spreads to the hyaline cartilages of the larynx, causing them to suppurate and melt with the formation of fistulas and sequestration. Diphtheria of the larynx (diphtheria croup) occurs more often in children. Due to the formation of fibrinous exudate in the area of the vocal cords and under them, increasing stridor, laryngostenosis develop, and pain in the larynx . Severe intoxication is noted. Laryngeal tuberculosis is often a complication of pulmonary tuberculosis. Patients' complaints of a sore throat, pain in the larynx, and hoarseness depend on the stage, location, extent and form of the process. When diagnosing, one should take into account the medical history, complaints, general condition of the patient, laboratory data (detection of Mycobacterium tuberculosis in sputum, results of tuberculin tests). A patient with suspected laryngeal tuberculosis should be referred to a phthisiatrician or otolaryngologist. Of the benign tumors, the most common are fibromas and papillomas . Angiomas and lymphangiomas are rarely observed. The main symptom of benign tumors of the larynx is hoarseness and pain in the larynx. To establish a diagnosis in all cases, a histological examination of the material obtained from a tumor biopsy is necessary.
Laryngeal cancer
Laryngeal cancer occurs predominantly in men, usually over the age of 40. Precancerous diseases of the larynx can be:
- leukoplakia;
- papillomas;
- keloid scars.
With cancer of the upper part (vestibule) of the larynx, there is soreness, a sensation of a foreign body, and pain in the larynx when swallowing, often radiating to the ear. With cancer of the true vocal cords, the most characteristic initial symptom is hoarseness .
With cancer of the lower larynx, slowly increasing difficulty breathing and hoarseness are more typical. As the tumor spreads to surrounding tissues and organs, these symptoms intensify, laryngostenosis gradually develops, metastases appear in the lymph nodes and nodes of the neck, and the general condition of the patients worsens.
When localized on the true vocal cords, voice formation is disrupted very early: first, the timbre of the voice changes, it becomes rough, and then hoarseness . Hoarseness most often forces the patient to see a doctor.
Later, as the tumor grows, the hoarseness intensifies, and the patient can only speak in a whisper. Along with this, another symptom develops, shortness of breath. In advanced stages, pain appears when swallowing.
With cancer of the epiglottis and arytenoid cartilages, the feeling of pain is preceded by a feeling of awkwardness or something foreign. In case of tumor disintegration and secondary perichondritis, pain in the larynx increases significantly. After some more time, hemoptysis, choking, and difficulty in passing food through the esophagus appear.
The decaying tumor emits a stench. Patients lose weight, become weaker, and cachexia increases. Clinical manifestations of laryngeal cancer are quite varied and depend primarily on the location and extent of the tumor lesion . Symptoms of cancer of the supraglottic region are scanty; at first, mainly unpleasant sensations or slight pain in the larynx are noted.
When the vocal folds are affected, the early and main symptom is gradually increasing hoarseness . Only cancer of the subglottic region occurs latently for a long time, difficulty breathing increases gradually and hoarseness increases slowly.
Other reasons
Foreign bodies enter the larynx mainly from the oral cavity. More often observed in children who have the habit of holding small objects in their mouths. A dangerous condition associated with small objects entering the respiratory tract: fish bones, needles, beads, coins. If the foreign body cannot be coughed out, it slips down into the trachea (all the way to the bronchi).
Larger objects can cause complete blockage of the lumen of the larynx - suffocation develops. With small foreign bodies, a convulsive cough, pain in the larynx, the face and lips turn blue, and hoarseness are observed. When completely blocked, suffocation occurs and death occurs. The main symptoms of gastroesophageal reflux disease are:
- heartburn;
- acute pain in the larynx;
- air burps;
- burning and feeling of pressure.
Zhennia occurs in the epigastric region 15-40 minutes after eating and is provoked by foods that stimulate the synthesis of acid and bile: fried, spicy food, sour juices, alcohol, especially dry red wine, carbonated drinks, consumption of soft-boiled eggs, radishes, radishes, large amounts of vegetable fat If you have pain in the larynx, seek help from an otolaryngologist, oncologist, or infectious disease specialist.