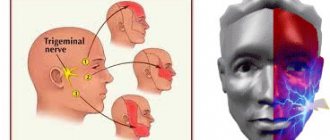
Leukoplakia - what is it?
Leukoplakia refers to the presence of small areas of altered mucosa. This nonspecific process can be found in any organ where there is a mucous membrane, but most often it occurs in the oral cavity and on the genitals.
We can talk about the problem as a precancerous condition, since it has the potential to develop into a malignant tumor.
With this nonspecific process, the appearance of an area of dense cells of the surface epithelium is observed. In a normal state, there is a regular process of death and exfoliation of the upper layers of the skin and mucous membrane. As the pathology develops, it disrupts it, thus the cells that have died do not disappear and form a multilayered whitish island.
Uterus and reproductive organs
The female reproductive system is represented by the mammary glands and pelvic organs.
The main function of these organs is procreation. The gonads produce regulatory substances that affect the development of the reproductive system and other organs. The most important structures are the ovaries, in which the maturation of female germ cells occurs. During ovulation, the reproductive cell leaves the ovarian follicle and enters the fallopian tube. The fusion of male and female reproductive cells in this organ leads to the formation of the rudiment of a new organism. The remaining stages of embryo development occur in the lumen of the uterus. The uterus is a hollow muscular organ located next to the rectum, vagina, ovaries and bladder. The uterine cavity is connected to the external environment through the cervical canal and the vaginal opening. The fallopian tubes allow the fertilized egg to migrate to the uterus. Attachment of the embryo to the inner layer (endometrium) of the organ is necessary for the formation of embryonic organs.
The main part of the cervix is the narrow cervical canal, which connects the vaginal opening to the uterine cavity. This anatomical structure is necessary for the transport of sperm into the fallopian tubes. The mucous membrane of the cervical canal contains a large number of glands that secrete a special fluid. Gynecologists include the functions of cervical mucus as protection against pathogenic microorganisms and ensuring the transportation of sperm. Smooth muscle and elastic fibers of the cervix provide expansion of the cervical canal during childbirth.
What does leukoplakia look like?
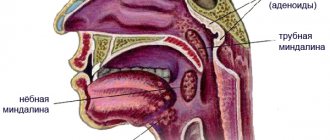
The disease can affect not only the oral cavity, but also other organs (esophagus, bladder, genitourinary organs, etc.) that have a mucous membrane, however, it is in the mouth that the lesion can be diagnosed earlier than in other places.
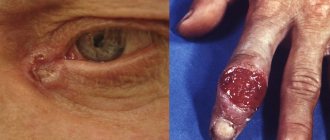
Foci of damage to the mucous membrane are characterized by plaques and growths of whitish or gray color, ranging in size from a few millimeters to three to four centimeters. During a quick examination of the oral cavity, plaques located under the tongue and on the walls of the cheeks can be quite difficult to notice. At the initial stage of the disease, the plaques practically do not rise above the rest of the surface of the mucous membrane, but later they can become hard, heterogeneous, ulcerated, and acquire sharp edges that cause discomfort.
Focal leukoplakia can form over months and even years, however, most often the lesions are visually determined within a couple of weeks after the onset of the disease. In this case, in most patients there is no pain, only a slight increase in the sensitivity of the affected area to temperature effects.
Causes
The exact causes of leukoplakia are unknown. Gynecologists associate the etiology of this disease with pathological external and endogenous influences. Thus, a significant increase in estrogen production against the background of progesterone deficiency can trigger the development of the disease. Hereditary factors play an important role in the formation of leukoplakia: certain genetic mutations can cause epithelial changes.
Possible reasons:
- Diseases of the endocrine system. The endocrine glands regulate the development of all organs, including the structures of the reproductive system. The greatest risk of developing cervical leukoplakia is associated with a disorder of the pituitary gland and ovaries. Diseases of the thyroid gland and adrenal glands can also be complicated by damage to the cervix.
- Chronic infections and inflammatory diseases of the pelvic cavity. In particular, human papillomavirus infection directly affects the condition of the cervical epithelium.
- Sexually transmitted infections including chlamydia, gonorrhea and herpes. Sexually transmitted diseases affect the condition of the external and internal genital organs.
- Mechanical damage to the cervical epithelium that occurs during trauma, diagnostic and therapeutic procedures. Artificial termination of pregnancy leads to tissue trauma.
- Mutation of the gene responsible for suppressing the growth of tumor cells. According to research, a mutation in the p53 gene, which controls cell development, leads to impaired tissue growth.
Normally, the outer lining of the cervix is represented by stratified non-keratinizing epithelium. Certain diseases can affect the internal structure of epithelial cells. Changes in the regulation of epithelial cells lead to keratinization and thickening of the outer layer of the membrane. It is assumed that one of the mechanisms of cell changes is the expression of a mutant gene.
What it is
It is believed that leukoplakia occurs against the background of chronic irritation of the oral mucosa and is a kind of protective reaction of the body. This is a local reaction and is not transmitted through contact with a sick person.
The disease is not so harmless, since it most often occurs shortly before the development of oral cancer. Many people mistakenly believe that leukoplakia itself is cancer, however, this opinion is incorrect. This disease affects the epithelial covering of the oral cavity in response to constant external irritants; vitamin deficiency, a decrease in the level of immunity and the presence of chronic foci of inflammation in the oral mucosa serve as an additional impetus for its development.
Leukoplakia of the oral cavity is a significant lesion of the mucous membrane of the lips, tongue, cheeks, upper and lower palate, manifested by keratinization (hardening) of the epithelial cover to varying degrees. Doctors usually classify leukoplakia as a disease that precedes the development of a tumor.
The greatest risk of developing this disease are men in the age group from 30 to 70 years, who abuse alcohol, smoke and wear dentures. Leukoplakia does not occur overnight, and its development can last for years.
Risk factors
In addition to the direct causes of cervical leukoplakia, gynecologists recognize the importance of certain forms of predisposition to the disease associated with heredity, individual history and a woman’s lifestyle.
Known risk factors:
- unprotected sexual intercourse;
- menstrual irregularities;
- drinking alcoholic beverages and smoking;
- radiation therapy of the pelvic organs;
- insufficient intake of vitamins and microelements from food;
- metabolic diseases;
- uncontrolled use of hormonal drugs;
- detection of leukoplakia or cervical carcinoma in a close relative.
Eliminating some of the risk factors listed above is an effective method of preventing the disease.
Leading specialists in the treatment of vulvar leukoplakia in the Southern Federal District
Ermolaeva Elvira Kadirovna is a well-known and recognized specialist in the North Caucasus in the treatment of leukoplakia of the vulva, vagina and cervix, diagnosis and treatment of kraurosis, lichen sclerosus, Keir's erythroplasia and other diseases of the vulva. One of the authors of the method of regenerating microinjections for the treatment of leukoplakia. Desperate people turn to her and women exhausted by suffering. Experienced gynecologist, physiotherapist-health resort specialist, ultrasound doctor.
Ermolaev Oleg Yurievich Candidate of Medical Sciences, gynecologist-endocrinologist with 25 years of experience and successful experience in the treatment of dysplasia, kraurosis and leukoplakia of the vulva Able to see relationships that elude others
About the doctors of the Clinic in detail...
| INTERNATIONAL RECOGNITION of the reputation and achievements of the Women's Health Resort Clinic in the development and implementation of effective and safe treatment methods and the quality of medical services provided is the AWARDING of the Women's Health Resort Clinic in Pyatigorsk with the SIQS International QUALITY CERTIFICATE in the field of medicine and healthcare. International Socratic Committee, Oxford, UK and Swiss Institute for Quality Standards, Zurich, SWITZERLAND. |
The resort women's health clinic is open 7 days a week and on holidays:
Monday - Friday from 8.00 to 20.00, Saturday, Sunday, holidays from 8.00 to 17.00.
Treatment of vulvar leukoplakia in Pyatigorsk by appointment no later than 3 days in advance by multi-channel phone number 8 (calls within Russia are free), or (for foreign calls).
| ONLINE information about the treatment of vulvar leukoplakia in Pyatigorsk can be found at REGISTER ONLINE for leukoplakia treatment here. REGISTER online for leukoplakia treatment here. You can buy a COURSE for treatment by phone or here. |
Booking a course
The doctors of the Women's Health Resort Clinic have gained EXTENSIVE EXPERIENCE in treating vulvar leukoplakia, vaginal leukoplakia, cervical leukoplakia using natural medicines and resort factors.
We accept women from all cities of Russia, near and far abroad.
The spa clinic for women's health facilitates the accommodation and accommodation of women, women with children and couples during examination and treatment.
ACCOMMODATION in Pyatigorsk is NOT INCLUDED IN THE PRICE of the treatment course and is paid separately.
About living conditions and transfer from Mineralnye Vody airport and Pyatigorsk railway station in detail in the article “Accommodation”.
If you need to book accommodation, please coordinate your arrival date no later than 7 days in advance.
We are at your complete disposal if you have any doubts or wishes.
Classification
There are two main types of cervical leukoplakia, differing in morphological and functional features. Determining the specific type of disease is possible only with the help of histological examination. Different morphological forms of leukoplakia differ in the risk of malignant degeneration.
Forms of the disease:
- Simple leukoplakia, characterized by coarsening of the outer layer of the epithelium and excessive cell division. Significant morphological changes in the cells of the basal layer are not detected.
- Proliferative leukoplakia. This form of the disease is characterized by a violation of cell specialization and the appearance of specific morphological changes. Proliferative leukoplakia is considered a precancerous condition.
Determining the form of the pathology is necessary to select treatment.
Consequences
Many patients, having received a similar diagnosis from a doctor, are interested in whether leukoplakia is dangerous. Most doctors consider simple forms of this disease to be safe and do not require special treatment. Leukoplakia in the initial stage has a favorable prognosis, especially if it is caused only by external irritants, and not by a functional disorder of the internal organs.
However, there are also frequent cases of precancerous leukoplakia - the danger of this form is clear to everyone. If atypical cancer cells are detected in the histological analysis of the obtained material, this type of disease requires immediate surgery. If left untreated, the consequences of leukoplakia at the cancer stage can be disappointing. After the operation and the end of the rehabilitation period, the patient is recommended to undergo periodic examinations and take a course of medications aimed at a speedy recovery.
Symptoms
In most cases, the disease does not manifest itself symptomatically. In itself, the coarsening of the outer epithelium of the cervix does not lead to dysfunction of the organ, so the pathology can remain undiagnosed for a long time. Typically, leukoplakia becomes an incidental finding during a gynecological examination.
Possible symptoms:
- discomfort during sexual intercourse;
- pain during menstruation;
- bloody issues;
- excess vaginal discharge.
The appearance of frequent uterine bleeding not associated with menstruation and pain may indicate the transformation of leukoplakia into a malignant tumor.
Diagnostics
If risk factors for the disease are detected, you must make an appointment with a gynecologist. During the consultation, the doctor will ask the woman about her complaints and examine her medical history. Then an initial examination of the genital organs is carried out, including palpation examination and the use of mirrors to assess the condition of the cervix. If suspicious changes are detected, the gynecologist prescribes instrumental and laboratory tests.
Additional diagnostic methods:
- Colposcopy is a method of visual examination of the cervix. The doctor asks the patient to sit in the gynecological chair. A colposcope equipped with optics and a light source is carefully inserted into the cervix through the vaginal opening. The gynecologist studies in detail the condition of the epithelium of the organ. Treatment of suspicious areas with iodine solution makes it possible to detect pathological changes in tissues. If necessary, the optics are replaced by a video camera, allowing the specialist to see a clear image of the organ tissue on the monitor. Colposcopy is a reliable and safe examination that does not require anesthesia.
- Scraping of cervical epithelial cells. During a colposcopy, the doctor inserts a special instrument into the organ cavity to collect cells from the suspicious area. Cytological examination of the obtained material in the laboratory makes it possible to evaluate morphological changes and determine the form of leukoplakia. Cytology is a reliable method for excluding malignant tissue degeneration.
- Cervical biopsy. If the epithelium is severely coarsened, the doctor cannot obtain cells from the lower layers of leukoplakia by scraping. In this case, a knife biopsy is the optimal diagnostic procedure. Using a special instrument, the specialist excises the required amount of tissue. Cytological examination of the biopsy is also necessary to exclude the growth of malignant cells. The procedure is performed under local anesthesia. If necessary, the gynecologist prescribes complete curettage of the epithelium of the cervical canal.
- Microbiological examination of the material. Tissue obtained by scraping or smear can be used to rule out infection. Special nutrient media give a specialist the opportunity to identify the causative agent of the disease.
- Blood analysis. In the treatment room, a nurse collects venous blood from a patient. Laboratory examination of the material is carried out to detect signs of inflammation and infection. Serological tests aimed at searching for specific immunoglobulins are necessary to exclude sexually transmitted diseases. If an HPV infection is suspected, sections of the DNA of the virus are searched using polymerase chain reaction (PCR).
The scope of diagnosis depends on the results of colposcopy and general examination. The main goal is to eliminate the risk of malignant tissue degeneration.
Treatment
The treatment method depends on the form of leukoplakia and the patient’s individual medical history. Due to the high risk of transformation of the pathology into carcinoma, it is recommended to remove the focus of the changed tissue. In some cases, the gynecologist prescribes drug therapy. Prescribed medications may include antibiotics and anti-inflammatory medications. Treatment of the root cause of the disease helps prevent relapse.
Pathology removal methods:
- Cryosurgery is the use of cold to destroy the affected epithelium. During the procedure, the patient is in a gynecological chair. After inserting the dilator into the cervix, the surgeon uses a special probe, the tip of which is cooled with liquid nitrogen. Destruction of leukoplakia takes 5-10 minutes. Cryosurgery is not accompanied by tissue trauma or severe pain.
- Radio wave destruction. A special device inserted into the cervix affects the tissue. This is a safe and fast treatment method with a low risk of complications.
- Other methods of minimally invasive removal of the disease, including chemical cauterization and argon plasma coagulation. The duration of rehabilitation after such interventions does not exceed 2 months.
If the gynecologist detects signs of malignant degeneration of leukoplakia, radical methods of surgical treatment are prescribed. The doctor needs to remove not only the pathological focus, but also the cells surrounding it. This is important to prevent abnormal cells from migrating into neighboring tissues.
Other methods of surgical treatment:
- Conization of the cervix. Using a special instrument, the specialist applies radio waves to the organ and removes the affected part of the cervix. This is a low-traumatic procedure that allows you to preserve reproductive function.
- Amputation of the cervix - removal of the affected segment of the organ. The disadvantage of this method is the high degree of tissue trauma, but the operation allows you to preserve the integrity of the reproductive system.
During treatment of the disease, the doctor asks the patient to abstain from sexual intercourse and taking hormonal contraceptives.
LEUKOPLAKIA OF THE CERVIX
The occurrence of cervical cancer in women of reproductive age is preceded by inflammatory processes of the uterus and appendages, menstrual dysfunction, and chemical and traumatic effects are of great importance. A comprehensive examination for FSM includes clinical, colposcopic, cytological, morphological, as well as bacterioscopic and bacteriological methods. Currently, many different methods of treating patients with cervical cancer have been proposed. The most effective methods of treating FSM today include the cryogenic method and especially high-intensity laser exposure. Uterine cervical leukoplasia (UCL) occupies a special place in the structure of diseases of the uterine cervix. Its etiology and pathogenesis has been so far controversial. The occurrence of UCL in reproductive females follows prior inflammations of the uterus and appendage, impaired menstrual function; chemical exposures and injuries are also of great importance. Comprehensive study in UCL involves clinical, colposcopic, cytological, morphological, bacterioscopic and bacteriological methods. Many different treatments for UCL have been proposed. At present, the most effective treatments are cryogenic therapy and especially high-intensive laser radiation.
V.N.
Prilepskaya - Prof., Doctor of Medical Sciences, Head of the outpatient department of the Scientific Center of Obstetrics, Gynecology and Perinatology (Director - Academician of the Russian Academy of Medical Sciences Prof. V.I. Kulakov), Russian Academy of Medical Sciences, Moscow
Prof. VN Prilepskaya, Dr. Sci., Head of Outpatient Department, Research Center of Obstetrics, Gynecology, and Perinatology, (Director Prof.VIKulakov, Academician of the Russian Academy of Medical Sciences), Russian Academy of Medical Sciences
L
Cervical neucoplakia (CMP) occupies a special place in the structure of cervical diseases, since the issue of its pathogenesis, benignity or malignancy of the course is still controversial. According to modern data, cervical cancer is a polyetiological disease and is based on many predisposing factors: previous infectious diseases, disorders of the immune status, hormonal homeostasis, traumatic effects on the cervix during childbirth, abortion, incorrect and inadequate treatment of cervical pathology and many others. Currently, the oncological aspect of gynecological diseases is considered inextricably linked with the endocrine function of the reproductive system. Data have emerged on the role of functional hormonal disorders in the pathogenesis of cervical diseases. Thus, the works of a number of authors have proven that the incidence of cervical diseases in patients with menstrual dysfunction is 5 times higher than among the general population [1]. Data on the frequency of leukoplakia in the structure of cervical diseases are contradictory [1–4]. Some researchers note a high incidence of this disease – from 11.7 to 12.5% [2, 5, 6]. According to M.Yu. Novikova [7], the frequency of cervical cancer is 1.1%, and in the structure of cervical diseases it accounts for 5.2%. And although this pathology does not occur very often, malignant transformation of stratified squamous epithelium (MSE), according to some researchers [2], is observed in 31.6% of patients with cervical cancer; in this regard, timely diagnosis and treatment of this disease is an important preventive measure and reducing the incidence of cervical cancer. The term “leukoplakia” (translated from Greek means “white plaque”) was first proposed by Schwimmer in 1887 and remains generally accepted to this day in Russian literature and clinical practice [2]. An analysis of foreign literature over the past 10 years has shown that the term “leukoplakia” itself in relation to lesions of the cervix is not used in some countries, while for leukoplakia of other localizations (vulva, oral mucosa) this term is widely used. Leukoplakia without cellular atypia, the so-called simple leukoplakia, is classified by foreign researchers as hyper- and parakeratosis [4], and leukoplakia with dysplasia atypia is classified as “cervical intraepithelial neoplasia” (CIN) [8 – 10].
Etiology and pathogenesis
In the etiology of FSM, it is customary to distinguish the following groups of factors: – endogenous (disturbance of hormonal homeostasis, changes in immune status); – exogenous (infectious, chemical, traumatic). In the 1960s and 1970s, the theory of hormonal genesis of underlying diseases of the cervix and leukoplakia in particular began to develop. As a result of functional disorders in the hypothalamus - pituitary gland - ovaries - uterus system, the ovulation process is disrupted. The consequence of anovulation is relative or absolute hyperestrogenism and progesterone deficiency, leading to the development of hyperplastic processes in target organs. The occurrence of cervical cancer in women of reproductive age is preceded by inflammatory processes of the uterus and appendages against the background of menstrual dysfunction such as oligomenorrhea in 35.5% of patients and by the type of defective luteal phase of the cycle (in 64.5%). According to M.Yu. Novikova [7], in patients with cervical cancer the function of the pituitary-ovarian system is impaired. Chemical and traumatic effects also play an important role in the occurrence of cervical cancer. It has been proven that more than 1/3 of patients with cervical cancer had previously received intensive and inadequate drug treatment for pseudo-erosion of the cervix, and 33% of patients with clinically significant leukoplakia had previously undergone diathermocoagulation [7]. Thus, patients with menstrual irregularities, previous inflammatory diseases of the genital organs, and a history of recurrent pseudo-erosions of the cervix should be included in the risk group for the occurrence of cervical cancer.
Clinical manifestations and diagnosis
Clinical examination data are of great importance. When analyzing anamnesis data, attention is paid to the nature of menstrual function (age at menarche, duration of the period of formation of menstrual function, rhythm of menstruation, etc.), the presence and outcome of pregnancies, the presence of a history of cervical pseudo-erosions, as well as the nature and effectiveness of previous therapy , duration of the FCM disease. Noteworthy is the asymptomatic course of the disease, as well as the absence of specific complaints. Only a small number of women complain of profuse leucorrhoea and contact spotting. A comprehensive examination for cervical cancer includes clinical, colposcopic, cytological, and, if indicated, morphological, as well as bacterioscopic and bacteriological methods. The most informative are extended colposcopy and morphological research methods. Extended colposcopy allows you to clarify the size and nature of leukoplakia, assess the condition of the integumentary epithelium of the vaginal part of the cervix. Depending on whether leukoplakia is detected only during colposcopy or is visible to the naked eye, colposcopically and clinically pronounced forms are distinguished. The colposcopic form includes “silent iodine-negative zones”, which can only be diagnosed using the Schiller test, and the clinically pronounced ones include “simple leukoplakia”, “base of leukoplakia” and “fields of leukoplakia”. Colposcopic forms of leukoplakia are described in various domestic and foreign guidelines on colposcopy [2, 3, 11]. Until now, the clinical-endoscopic-morphological classification of I.A. is generally accepted for clinicians. Yakovleva and B.G. Kukute [5], according to which simple leukoplakia without atypia is classified as background processes, and leukoplakia with atypia is classified as precancerous conditions. Some authors classify simple leukoplakia as hyper- and parakeratosis, and leukoplakia with cellular atypia as CIN of varying severity, which depends on the severity of atypia. Simple leukoplakia is a thin white film that can easily peel off, or dense lumpy plaques with clear contours. The external manifestations of simple leukoplakia depend on the thickness of the keratin layer. After its removal, shiny pink areas are visualized, indicating the true size of the lesion, the Schiller test is negative, the vessels are not visible, since leukoplakias are devoid of vessels. The base of leukoplakia colposcopically looks like an iodine-negative area covered with red dots of equal size. Red dots represent connective tissue papillae in stratified squamous epithelium, in which loops of capillaries are visible. Mosaic or fields of leukoplakia during colposcopy look like polygonal areas separated by red threads of capillaries, creating a mosaic pattern. When treated with acetic acid, the mosaic pattern becomes more distinct, the Schiller test is negative. For the purpose of early diagnosis of cervical cancer, impression smears from the surface of the integumentary epithelium of the cervix are examined. It is convenient to take material for cytological examination with an Eyre spatula or a special cervical brush. At the same time, smears are taken from the vaginal part of the cervix, transition zone and the lower third of the cervical canal. However, due to the presence of the stratum corneum on the surface of the MPE, cells with dyskaryosis from the deep layers, where differentiation disorders, proliferation and atypia are possible, are not included in the smears. Dyskaryosis is characterized by the following features: an increase in the nuclear-cytoplasmic ratio, size, change in the shape of the nuclei, unevenness of their contours, hyperchromasia, multinucleation and the presence of numerous nucleoli in the nuclei. With simple leukoplakia, the impression smears contain clumps of keratin, accumulations of superficial cells devoid of nuclei, the cytoplasm of which is stained yellow or orange using the Papanicolaou method. The smears also contain layers of polygonal keratinizing cells with a pyknotic nucleus of irregular shape - dyskeratocytes. The main method for diagnosing cervical cancer is a morphological examination of a cervical biopsy.
For its high-quality implementation, it is necessary to perform a targeted knife biopsy under colposcopy control from the affected areas of the cervix. Simultaneously with the biopsy, the mucous membrane of the cervical canal is scraped. The need for revision of the cervical canal is due to the fact that the pathological process can develop not only on the vaginal part of the cervix, vagina and vulva, but also in areas of squamous metaplasia of the mucous membrane of the cervical canal. Therefore, to exclude precancerous changes and malignant transformation of the epithelium, it is necessary to include curettage of the endocervical mucosa in the complex of diagnostic measures. The morphological picture of leukoplakia is characterized by the following structural changes in the MPE: •thickening of the integumentary epithelium, mainly due to an increase in the number of cells of the spinous layer while maintaining their complexity; it may be caused by acanthosis - immersion of epithelial layers into subepithelial connective tissue; •the presence of a stratum corneum on the surface of the epithelium, which is normally absent; •the presence of a granular layer, which is located under the stratum corneum and is represented by 2–3 rows of cells, the cytoplasm of which is filled with a moderate amount of basophilic granules; •scattered or focal lymphoid infiltration of subepithelial connective tissue. In areas of leukoplakia, glycogen is always absent. Also, with leukoplakia, parakeratosis is quite common - incomplete keratinization of the MPE. In this case, the surface layer of MPE is represented by several rows of flattened cells, elongated parallel to the base, with small pyknotic nuclei and oxyphilic cytoplasm. Under the parakeratosis, the granular layer is absent. In areas of parakeratosis, glycogen is either not detected or traces of it are visible. In the histological assessment of leukoplakia of any localization, the presence or absence of cellular atypia in the lower layers of the MPE is very important. As already mentioned, leukoplakia without atypia is a benign lesion of the cervix and refers to background diseases, and in the presence of atypia - to precancerous conditions, and is also classified as cervical dysplasia depending on the severity of atypia. In recent years, microcolpohysteroscopy has been used for a more detailed examination of the cervix and cervical canal. The advantages of this method are the possibility of atraumatic passage of the cervical canal under constant visual control, without any anesthesia. Microcolpohysteroscopy allows you to assess the condition of the walls of the cervical canal in patients with cervical cancer, detect atypical cells, and perform a targeted biopsy.
Treatment
Currently, many different methods of treating patients with cervical cancer have been proposed. From the arsenal of means available to practitioners, the most commonly used are diathermocoagulation, cryogenic exposure, high-intensity laser radiation, and various medicinal methods based on the general or local effect of drugs on the pathologically altered cervix. Until now, clinicians have difficulty managing and treating such patients. It should be emphasized that when FSM is combined with inflammatory processes of the vulva and vagina of various etiologies, it is first necessary to eliminate the inflammatory process, for which antibacterial drugs of various spectrums of action, antitrichomoniacal, antifungal, antiviral, antichlamydial agents should be prescribed according to the regimens generally accepted in clinical practice in accordance with preliminary data bacterioscopic and bacteriological examination, as well as the results of examination for chlamydia and viruses. Doctors should be warned against using products that affect tissue metabolism (sea buckthorn oil, rosehip oil, ointment containing aloe, etc.). These drugs can enhance proliferative processes and the occurrence of cervical dysplasia. Chemical coagulants are still used for the treatment of LSM. Of this group of drugs, Solkovagin deserves special attention, which is a mixture of organic and inorganic acids and has a coagulating effect selectively on the columnar epithelium. The penetration depth of the drug reaches 2.5 mm, which is sufficient for coagulation of the pathological area of the ectocervix. Treatment with solkovagin is painless and ensures complete destruction of the pathological focus due to a sufficient depth of penetration. The effectiveness of treatment of simple LSM with this method in young nulliparous women was 74.3% [1]. Diathermocoagulation is still widely used in everyday practice. However, according to long-term clinical observations, this method produces unwanted side effects. These include: implantation endometriosis, bleeding at the time of scab rejection, exacerbation of inflammation of the uterine appendages, menstrual dysfunction, pain syndrome, prolonged course of reparative processes, frequent relapses of the disease. The most effective methods of treating FSM today include the cryogenic method and especially high-intensity laser exposure. Cryotherapy causes necrosis of the pathological focus due to the influence of low temperature. It is carried out by contact method, most often once, its duration is determined by the nature and extent of the pathological process and ranges from 2 to 5 minutes. The advantages of this method include the painlessness of the procedure and the possibility of use on an outpatient basis. The effectiveness of this treatment ranges from 54 to 96%. One of the disadvantages of the method is the recurrence of the pathological process, especially in patients with menstrual irregularities. One of the most modern and effective methods of treating cervical cancer is the use of high-intensity laser. The advantage of the CO2 laser is its ability to contactlessly, painlessly, aseptically, bloodlessly evaporate, burn and coagulate pathological tissues, forming a thin coagulation film on the wound surface that prevents infection from penetrating into the underlying tissues. As a rule, laser coagulation is performed on an outpatient basis without prior anesthesia in the first half of the cycle (on the 4th – 7th day). Before laser exposure, the cervix is treated with Lugol's solution to more accurately determine the area of pathological tissue to be removed. In case of extensive damage to the cervix with the spread of leukoplakia to the fornix and vagina, it is advisable to use two-stage laser radiation: Stage I - laser coagulation of the vaginal part of the cervix; Stage II – removal of the pathological epithelium of the vagina (performed during the next menstrual cycle). Complete epithelization occurs on the 16th – 40th day, depending on the prevalence and extent of the process. In cases of combination of leukoplakia with pronounced deformation and hypertrophy of the cervix, it is advisable to use surgical methods of treatment - knife or laser conization, wedge-shaped or cone-shaped amputation of the cervix, reconstructive plastic surgery with restoration of the normal anatomy of the cervical canal. Thus, currently in the arsenal of doctors there is a sufficient number of methods for treating cervical cancer, which, of course, should be used differentiatedly. However, none of these methods are perfect. It should be emphasized that preference for this pathology should be given to laser coagulation.
Prevention
The principles of prevention of cervical cancer include rational treatment of previous background processes in the cervix, excluding the traumatic effects of diathermocoagulation and chemical coagulates on the ectocervix, as well as timely treatment of inflammatory processes of the genital organs and menstrual irregularities. Patients with a history of exposure to the cervix with diathermocoagulation and chemical coagulates due to previous pathological processes require dynamic monthly colposcopic monitoring, especially during the first year after local exposure to the cervix.
Literature:
1. Prilepskaya V.N., Kostava M.N., Nazarova N.M. // Obstetrics. and gin. 1992. - No. 12. — P. 62-5. 2. Vasilevskaya L.N. Colposcopy. – M.: Medicine, 1986. – 157 p. 3. Prilepskaya V.N., Rogovskaya S.I., Mezhevitinova E.A. Colposcopy. M.: Medicine, 1997. – 108 p. 4. Boon ME., Suurmeijer AHH. The PAP Smear. Coulomb Prees Leyden 1991;77-82. 5. Yakovleva I.A., Kukute B.G. // Arch. Pat. 1977. – T. 39. – No. 1. — P. 18-25. 6. Burk CE., Henderson PH. Amer J Obstret Gynec 1963;21,(3):279-90. 7. Novikova M.Yu. Author's abstract. diss. Ph.D. honey. Sciences - 1995. 8. Burghardt E. Kolposkop. Stuttgart: New York, 1981; 253. 9. Cartier R. Practical Colposcopy. – Gustav Fischer Verlag: Stuttgart, New York, 1984;114-438. 10. Coupez F J Gynecol Obstet 1976;5 (3):177-8. 11. Prilepskaya V.N., Novikova M.Yu., Ezhova L.S. .// Obstetrics and gyne. – 1994. – No. 3. — P. 6-9.
Prevention and prognosis
In most cases, the prognosis is favorable. The absence of human papillomavirus infection and dysplasia indicates a low risk of malignant tissue degeneration. Surgical intervention not only eliminates the risk of organ malignancy, but also preserves reproductive function. After treatment, the gynecologist regularly conducts examinations to eliminate the risk of relapse.
Simple medical recommendations can reduce the likelihood of leukoplakia and other diseases of the reproductive system. Prevention methods are aimed at changing lifestyle and eliminating negative external factors.
Basic methods of prevention:
- use of hormonal drugs only under the supervision of a physician;
- regular gynecological examinations;
- keeping a calendar of the menstrual cycle and contacting a doctor if disorders occur;
- refusal of alcoholic beverages and cigarettes;
- timely treatment of chronic diseases of the genital and endocrine organs;
- using a latex condom;
- sexual intercourse only with a trusted partner (HPV infection can be transmitted even when using a condom).
A consultation with a gynecologist or oncologist will help a woman learn more about the risk factors for leukoplakia and treatment methods for this disease. If necessary, the doctor immediately conducts an examination and excludes the presence of suspicious changes in the cervix.
Pregnancy with leukoplakia
Before you start planning a pregnancy, you need to undergo an examination and a course of treatment prescribed by your doctor.
If the pathology is detected during pregnancy, treatment is postponed until the postpartum period. It should be borne in mind that leukoplakia does not affect the course of pregnancy and the development of the baby, however, against the background of a hormonal surge, progression of cervical cancer is possible. In this regard, the expectant mother should be under close medical supervision.
In most cases, leukoplakia is not a contraindication to natural childbirth, however, if the pathological process spreads to the vagina and vulva, the obstetrician-gynecologist may recommend a cesarean section.