Causes of pimples in the mouth
70% of red, white or pinkish rashes in the oral cavity, including on the tongue, indicate the presence of a serious dental disease. The asymptomatic course of the disease does not mean that the “trouble” will go away on its own. However, prescribing treatment on your own, guided by the advice of friends or recommendations from the Internet, is dangerous.
Important!
In principle, there cannot be acne on the tongue. Purulent skin rashes develop due to inflammation of the sebaceous glands, which are not present in the mouth. Accordingly, we call those pimples that appear in the oral cavity “pimples” by analogy. Just by external similarity.
There are several reasons for the appearance of irritations that visually resemble pimples:
- mechanical damage. A prick with a fish bone, a scratch, a burn from hot coffee can provoke a similar pathology;
- allergy. Not necessarily to foods; a seasonal allergic reaction is possible, manifesting itself in such an unusual way;
- viral and infectious diseases. Herpes, rubella, scarlet fever and ARVI sometimes manifest themselves as rashes in the mouth;
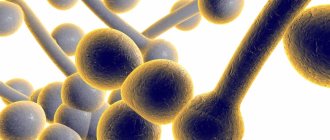
- fungal infection (candidiasis);
- stomatitis. Usually, with stomatitis, pimples first appear on the gums, but sometimes red spots with a whitish halo, which react sharply to touch or spicy/hot food, form over the entire lingual surface.
There is no point in waiting until diseases become chronic. In 98% of cases, such pathologies are treated quickly and inexpensively, if you do not neglect the condition and do not self-medicate.
Causes of white plaque on the tongue
The reasons that cause a white coating on the tongue include:
- poor oral hygiene;
- medications (for example, long-term use of antibiotics);
- smoking;
- excessive consumption of alcoholic beverages;
- viral infections;
- diseases of the oral cavity (oral candidiasis (thrush), leukoplakia, lichen planus, geographic tongue (desquamative glossitis));
- chronic diseases (hypothyroidism, diabetes, syphilis);
- immunodeficiency conditions (HIV/AIDS);
- heat;
- improper use of an inhaler in the treatment of asthma, COPD;
- mechanical injuries to the oral mucosa caused by sharp edges of the teeth when damaged by caries or chips, dentures, piercings in the mouth;
- burns of the oral mucosa caused by too hot food or liquid;
- chemical injuries to the oral cavity;
- xerostomia (dry mouth);
- breathing through the mouth;
- a diet containing soft and pureed food, absence of coarse fibers in food;
- oral cancer, tongue cancer;
- radiation therapy of malignant neoplasms of the maxillofacial region.
The appearance of a pimple on the tongue: diseases and treatment
The most harmless reason for the appearance of a pimple on the tip of the tongue is mechanical damage. Regular antiseptic treatment is enough to get rid of the problem. To relieve inflammation, you can use decoctions of sage and chamomile. A prerequisite is not to touch the wound with your hands, as you risk causing a more serious infection.
Allergy
It usually manifests itself as a scattering of small pimples throughout the tongue plate; if treatment is not addressed immediately, the pathology penetrates the root of the tongue, the frenulum and affects the larynx.
When should you see a doctor if you have a white coating on your tongue?
White coating on the tongue is a symptom, not a disease, so it is necessary to find out the cause of plaque formation from a specialist (especially if it is accompanied by discomfort, pain and burning in the mouth, the plaque persists for more than several weeks, ulcers form, chewing and swallowing are difficult), and undergo diagnostics and treatment of the disease causing such symptom. Depending on the problem, the doctor will prescribe antifungal drugs, local glucocorticosteroid therapy, antibiotic therapy and other treatment methods.
Often, a white coating on the tongue goes away on its own (for example, caused by ARVI) within a few weeks. Don’t forget to take proper care of your oral cavity: brush your teeth regularly with a soft-bristled brush, use a special scraper on your toothbrush to clean your tongue, floss, mouthwash, drink plenty of water, try to eat healthy and balanced, give up bad habits, eat regularly Visit your dentist for preventive examinations (at least once every six months) and treatment.
Treatment Options
Treatment is closely related to the cause of the condition. Possible treatment regimens:
- antibiotics + antisecretory drugs + histamine receptor blockers + proton pump inhibitors for peptic ulcer disease;
- antifungal agents in the form of capsules, tablets or drops for candidiasis;
- opening the salivary ducts and removing blockages;
- correction of hormonal disorders with hormone replacement drugs;
- anti-inflammatory drugs and local antimicrobial agents for glossitis;
- infusion therapy and oral rehydration solutions for dehydration;
- antibiotic therapy for acute tonsillitis;
- antiretroviral therapy for immunodeficiency due to HIV.
The positive effect of treatment occurs immediately or after 3–5 days. If there is no improvement, a change in therapy or re-examination may be necessary.
There is no need to live with pain in the tongue and endure it, hoping for self-healing. It is better to consult a doctor in a timely manner, discover the cause and remove it, than to wait for serious complications.
Read also: Why does the tongue have a white coating?
Dear patients! Remember that only a qualified doctor can make an accurate diagnosis, determine the causes and nature of the disease, and prescribe effective treatment. You can make an appointment with our specialists or call a doctor at home by calling 8-(4822)-33-00-33
Be healthy and happy!
Manifestations of diseases of internal organs on the mucous membrane of the mouth, tongue and lips
Diseases of the mucous membrane (MU) of the mouth, tongue and lips are one of the important and complex areas of practical medicine. Patients often find themselves in difficult clinical situations when they receive untimely and inadequate care. The fact that the human body is a complex, hierarchical, dynamically self-governing formation, the stability of which is due to the simultaneous functioning of a number of organs and systems, began to escape the attention of the doctor.
The existing relationships between lesions of the mucous membrane of the mouth, lips, tongue and systemic pathology should alert both patients and dental and somatic doctors. In the medical literature, a large group of tongue diseases are presented that occur separately, without affecting other parts of the oral cavity: desquamative glossitis (“geographical” tongue), black (“hairy”) tongue, folded tongue, rhomboid glossitis [1].
Changes in the condition of the mucous membrane of the mouth and tongue can occur and be detected both before other clinical manifestations of systemic diseases, and simultaneously with them. In many systemic (somatic, general) diseases, the oral mucosa reacts with the appearance of various types of disorders: disorders of tissue trophism, bleeding, swelling, dyskeratosis . Some manifestations of pathology in the mucosa of the mouth and tongue clearly indicate one or another type of organ or systemic disorder and are of great diagnostic value. However, in most cases, despite the different etiology and pathogenesis, the manifestations of systemic diseases on the oral mucosa are not specific in nature and are characterized by similar, sometimes outwardly identical clinical signs, which creates difficulties in their recognition.
Often occurring lesions of the oral mucosa due to diseases of the gastrointestinal tract, cardiovascular system, endocrine pathology, deficiency of vitamins (especially group B), macro- and microelements can attract the attention of specialists in various fields. Since changes in the mucous membranes of the mouth and tongue can occur and be detected earlier than other clinical manifestations of systemic diseases or simultaneously with them, patients themselves often turn to a dentist. In turn, gastroenterologists, endocrinologists, cardiologists, and hematologists can involve a dentist for consultation and joint supervision of patients with lesions of the oral mucosa, lips and tongue.
In this regard, we consider it necessary to share our clinical observations. This message may be useful to specialists whose professional interests relate to the diagnosis of these diseases and the treatment of such patients. Our previous publications were devoted to these issues [2–10]. The latest report [11] provided data on cancer screening for diseases of the oral mucosa, tongue and lips.
During our many years of clinical practice, changes in the CO of the mouth, tongue and lips were observed in the pathology of various organs and systems of the body, and metabolic disorders. Lesions of the mucous membranes of the mouth, lips and tongue are most often found in diseases of the gastrointestinal tract. In this case, ulcerative, aphthous and necrotizing stomatitis develop. The best studied in this regard are language changes characterized by a number of features:
- coated tongue (Fig. 1), which is detected most often (with exacerbation of gastritis, gastroesophageal reflux disease, peptic ulcer, pancreatitis, enteritis and colitis, the amount of plaque increases);
- swelling of the tongue, diagnosed by tooth marks on its lateral surfaces, usually associated with enteritis and colitis;
- changes in the papillae of the tongue, manifested in the form of hyperplastic and atrophic glossitis;
- desquamation of the epithelium (sometimes in this case they talk about desquamative glossitis (Fig. 2), which some authors regard as an “independent disease of the tongue”);
- paresthesia and disorders of taste sensitivity, often accompanying not only diseases of the digestive system, but also developing as a result of an imbalance of vitamins and pathology of the autonomic nervous system.
Rice.
1. Coated tongue in a patient with chronic pancreatitis in the acute stage. Rice. 2. Desquamative glossitis in an 82-year-old patient suffering from peptic ulcer localized in the pylorus, who underwent radiation therapy for lung cancer and surgery for cancer of the rectosigmoid angle. Damage to the mucous membrane of the mouth, lips and tongue is observed with a deficiency of vitamins and microelements. The most common deficiencies in clinical practice are B vitamins and iron.
Pain, numbness, burning in the tongue, in the gums and lips are observed with hypovitaminosis B12, which is accompanied by neurological disorders and changes in hematopoiesis. Both with iron deficiency anemia and with latent iron deficiency, changes in the CO of the mouth, tongue and lips are caused by manifestations of tissue iron deficiency (sideropenia) . Patients (usually young girls and women) complain of perversion of taste sensitivity, paresthesia, burning of the tongue, pain and swelling in the tongue, sometimes difficulty swallowing dry and solid food, and choking. With severe sideropenia, the tongue, due to atrophy of the filiform and mushroom-shaped papillae, becomes smooth (“polished”, “varnished”), angular cheilitis develops, folds on the back of the tongue and trophic changes in the mouth are sometimes observed. It should be remembered that the appearance of symptoms of sideropenia often precedes a decrease in hemoglobin levels and can persist even after correction of anemia if iron therapy is insufficient.
Pain, numbness and burning in the tongue, in the gums, lips are observed with hypovitaminosis B12, which is accompanied by neurological disorders and changes in hematopoiesis (B12-deficiency anemia), so the mucus of the mouth is pale. Bright red areas of inflammation appear on the tongue, reacting to the intake of acidic foods and medications. These lesions are often localized along the edges and at the tip of the tongue, sometimes involving the entire tongue (“scalded” tongue) (the so-called Hunter-Meller glossitis). Often ulcerations and petechiae develop on the tongue. Such changes can spread to the gums, mucous membranes of the cheeks, soft palate, and less commonly to the mucous membranes of the pharynx and esophagus. Subsequently, the inflammatory phenomena subside, and the papillae of the tongue atrophy. The tongue becomes smooth and shiny (“varnished” tongue; Fig. 3).
Rice. 3. “Lacquered” tongue in a patient with B12-deficiency anemia.
With relapses of the disease, along with atrophic changes, hyperplasia of the papillae at the root of the tongue develops (hypertrophic papillitis). At the same time, leukokeratosis of the tongue and lip mucosa may be observed.
Vitamin B1 deficiency is accompanied by hyperplasia of the fungiform papillae of the tongue, paresthesia and allergic reactions of the oral mucosa. Hypovitaminosis B2 is manifested by a peculiar change in the skin, red border of the lips, mucous membrane in the corners of the mouth (angular stomatitis), oozing, maceration of the epithelium. A superficial form of desquamative glossitis is noted (triad: dermatitis, cheilitis, glossitis). With hypovitaminosis B6, symptoms of a disorder of the nervous system (polyneuritis) and the gastrointestinal tract, angular stomatitis, cheilitis, and glossitis are observed.
Lesions of the oral mucosa in diseases of the cardiovascular system are observed in more than half of patients with this pathology, in which the following are detected:
- swelling and cyanosis of the mouth and lips; in case of myocardial infarction, swelling of the tongue may be accompanied by the appearance of erosions, ulcers and “cracks”;
- vesical-vascular syndrome - the appearance (usually in older women suffering from arterial hypertension) of dense blisters (after opening, erosions form) with hemorrhagic contents on the mucous membrane of the soft palate, the lateral surfaces of the tongue, and the cheeks. It is necessary to differentiate this syndrome from pemphigus and erythema multiforme;
- ulcerative-necrotic lesions of the mouth with the formation of trophic ulcers in the absence of a pronounced inflammatory reaction in the surrounding tissues. We observed a patient with necrosis and sequestration of the body and branch of the mandible. These lesions must be differentiated from: traumatic ulcers, malignant tumors, Vincent's ulcerative necrotizing stomatitis, necrotic lesions of the mouth due to blood diseases.
The most common endocrine pathology in dentist practice is diabetes mellitus. There is a direct relationship between the severity of inflammatory changes in the oral mucosa and the course of the disease, its duration and the age of the patient. With a short duration of diabetes, the oral mucosa becomes hyperemic, swollen, and bleeds. With increasing duration of the disease, hyperkeratosis of filiform papillae and hyperplasia of fungiform papillae most often develop. The tongue is coated; hyperemic mushroom-shaped papillae in the form of reddish dots rise along the entire back of it.
The dentist is responsible for diagnosing the early manifestations of “general” diseases, conducting a thorough examination of the patient through the efforts of somatic doctors. Folding and an increase in the size of the tongue are often noted; a combination of tongue folding with hyperkeratosis of the filiform papillae or, conversely, with their desquamation (diffuse or focal) and dryness of the mucous membrane of the tongue is possible. There is a “geographical” language. Teeth imprints are identified on the lateral surface of the tongue. With decompensation of diabetes, decubital ulcers are possible and in almost all patients changes in the lips are detected: dry mouth and red border of the lips in combination with cracks, jams, crusts, bright hyperemia, especially pronounced in the Klein zone, angular cheilitis. In the diabetes compensation phase, dry mouth and angular cheilitis disappear.
Changes in the CO of the tongue are more stable, remaining in the phase of decompensation and compensation. Oral candidiasis often develops.
Basics of medical tactics for lesions of the mouth, lips and tongue:
- For rational treatment of diseases of the mouth, lips and tongue, a thorough examination of the patient and contact between the dentist and other specialists is required, first of all, with the therapist, as well as specialized specialists - gastroenterologist, endocrinologist, hematologist, cardiologist.
- An axiom for the dentist should be the elimination of all unfavorable irritating factors in the oral cavity in the patient, which can support and provoke the development of the pathological process. It is unacceptable to use the so-called cauterizing agents and long-term use of the same mouthwashes.
- Treatment of diseases of the oral mucosa must be carried out in compliance with the principles of bioethics; these diseases must be considered from the standpoint of the state of the whole organism, therefore, in most cases, one cannot limit oneself only to local effects on the lesions of the mucous membrane carried out by the dentist.
- Treatment should begin only after at least a preliminary diagnosis has been established and meet the following requirements:
- be comprehensive;
- provide a pathogenetic approach;
- do not violate the anatomical and physiological properties of oral mucosa;
- eliminate the pain factor;
- help optimize the epithelization of lesions;
- provide for the active involvement of the patient in performing medical procedures at home.
In some diseases, changes in the color and general appearance of the oral mucosa and surface of the tongue do not have independent diagnostic significance. However, in combination with other symptoms, the appearance of the lips, tongue, and oral mucosa can help clarify the diagnosis. The prognostic significance of changes in organs and tissues of the oral cavity is great. The dentist is responsible for recognizing and diagnosing early manifestations of “general” diseases and conducting a thorough examination of the patient through the efforts of somatic doctors. We are confident that timely and correct assessment of the described conditions in the practice of doctors of other specialties is very necessary and advisable.
Literature
- Danilevsky N. F., Leontyev V. K., Nesin A. F., Rakhniy Zh. I. Diseases of the oral mucosa. - M.: OJSC "Dentistry". — 271 p.
- Tsepov L. M., Mikheeva E. A., Nesterova M. M. Erosive and ulcerative lesions of the mucous membrane of the mouth, tongue and lips. Tactics of a dentist // Dental South. - 2009. - No. 8 (68). — P. 10-13.
- Tsepov L.M., Nikolaev A.I., Petrova E.V. et al. Symmetrical recurrent decubital ulcers of the mucous membrane of the lower lip in a patient with facial paraspasm // Dental South. - 2007. - No. 7 (56). — P. 28-29.
- Tsepov L. M., Tsepova E. L. Diagnostic value of changes in the lips, oral mucosa and tongue in various diseases and pathological conditions // Dental South. - 2010. - No. 6. - P. 14-16.
A complete list of references is in the editorial office.
Diagnostics
An in-person examination by a dentist is enough to detect the problem. Sometimes a doctor can immediately diagnose and prescribe treatment. But if the disease is not of a dental nature, additional examination will be required.
For diagnostic purposes the following is carried out:
- general blood test to identify an infectious process;
- FGDS for detection of peptic ulcer;
- biochemical blood test for glucose content and determination of hormone levels if endocrine disorders are suspected;
- examination by a neurologist and conducting tests to diagnose damage to the nervous system;
- blood test for HIV and hepatitis B, C to find the cause of immunodeficiency;
- examination by an otolaryngologist to detect acute tonsillitis (tonsillitis).
Carrying out all types of diagnostic procedures is not necessary; often the cause is determined at the initial stage. Based on the results of the examination, a treatment regimen is selected.
More rare situations
Yellow spots on a child’s tongue may indicate diseases of the digestive system1. Usually the problem manifests itself in the formation of a dense coating on the base of the tongue, which is difficult to remove. The cause should be sought with the help of a gastroenterologist.
Blue areas are extremely rare in childhood, as they signal problems with the cardiovascular system. Also, dark blue spots may just be hemangiomas that do not require any correction.
Bald spots are areas where taste buds are missing3. The child does not feel them, and they cannot be treated in any way, since the death of the papillae is irreversible. The main task of parents is to determine the reason for the formation of such areas.
What does the tongue look like normally?
In the absence of health problems, the child’s tongue looks moist, evenly pink, without areas of redness or swelling1. In some cases, parents may see plaque due to the following reasons:
- Insufficient and irregular oral hygiene.
- Eating food with coloring substances (lollipops, chocolate, persimmons, beets, carrots, ice cream, etc.).
- Using seasonings that have a coloring effect (curry) in cooking.
- Taking medications with a coloring effect (iron preparations, activated carbon, iodine sprays, solutions with furacillin and tannins).
- Excessive amounts of fatty foods in the diet.
Whitish spots on the tongue of an infant may appear due to the curdling of mother's milk in the mouth or minor regurgitation.