Main types of tooth movement
1. Corpus: the root and crown of the tooth move the same distance in the same direction a. mesial-distal movement = parallel movement (or right-left when looking at the tooth from the lips/cheeks) b. vestibulo-oral movement = narrowing/widening of the dentition (or back and forth if looking at the tooth from the lips/cheeks) c. dentoalveolar elongation/intrusion = extrusion/intrusion (or up-down)
2. Rotational: rotation around its axis
3. Oblique-rotational: the root and crown of the tooth move different distances in different directions a. mesial-distal tilt (angulation or right-left tilt) b. vestibulo-oral tilt (inclination = torque or forward-back tilting)
Significant torque
Torque is a collective concept. Let's look at it from 3 points of view.
1. From a clinical point of view, inclination of the tooth crown is the third key to correct occlusion according to Andrews. Inclination (or torque) is the angle formed between the perpendicular to the occlusal plane and the tangent to the middle of the vestibular or buccal surface of the clinical crown of the tooth.
The torque values are determined in absolute values of degrees of deviation from the coordinate line and are positive for the vestibular inclination of the teeth (outward) or negative for the oral inclination (inward).
The inclination of teeth to the vestibular side or the arrangement of teeth with a positive torque is called protrusion or proclination, the inclination of the teeth to the oral side or the arrangement of teeth with negative torque is called retrusion or retroclination.
2. From the point of view of the structure of the bracket, torque is the inclination of the bracket groove relative to the base.
Torque values are determined in absolute values of degrees of deviation from the plane perpendicular to the base. For the upper jaw they are positive when tilted downwards or negative when tilted upwards. For the lower jaw, it’s the other way around: negative when tilted down or positive when tilted up.
3. From the point of view of biomechanics, the term torque (from Latin torqueō) means “to twist, torque (in mechanics).” Torque or moment of a force couple characterizes the rotational action of a force on a rigid body. In this definition, torque is measured in N×mm or g×mm.
During treatment, torque is represented by twisting a rectangular arc in a groove.
Torque movement also refers to the movement of the tooth root or such movement of the tooth in which the root moves more than the crown.
Andrews' six keys of occlusion
Occlusion keys in orthodontics include 6 indicators. They were first described in 1872. Andrews developed six indicators of an ideal bite, for which he needed to study the condition of the oral cavity of 120 people. Today, the Andrews classification is actively used and makes it possible to determine the patient’s bite.
First
The first occlusal key evaluates the condition of the molars. They are located in the sixth position, if you count from the central point of the dentition. The first key determines the closure of the upper molar with the antagonist tooth. Normally, its distal cusp should be in contact with the lower molar number 2. It slopes distally. During closure, full contact is ensured between the lower and upper jaws.
Second
Evaluates angulation of dental crowns. The longitudinal axes have the correct ratio. With full contact, the long axis of the gingival part is located distal to the occlusal part. Depending on the name of the tooth, the degree of inclination changes.
Third
Evaluates the position of the tooth relative to its vestibular part and its inclination. On the upper incisors there is a labial location of occlusion in relation to the gingival zone. The remaining teeth are located lingually in relation to the gingival zone. If you look at the upper jaw, the lingual inclination of the molars will be more pronounced than that of the canines.
Fourth
The position of the teeth in the row relative to the axis is assessed. Normally, they should be located in an even arc, one after the other. When the axis changes, deformation is noted. If rotation is present in the incisors, the arc shortens and becomes flatter. If there is a turn in the premolars or molars, then the arch lengthens. In both cases, the contact between the lower and upper jaw is disrupted, and the occlusion is deformed.
Fifth
The density of the dentition is considered. Normally, a person should not have gaps, which in dentistry are called diastemas and tremata. If there are gaps, the patient’s load on the masticatory muscles is disrupted. Frequent causes of deformation are bad habits, impaired respiratory function and other conditions.
Sixth
The Spee curve is considered. Normally, it should not be more than two millimeters. The occlusion between the cusp of the lower second molar and the central incisor on the lower jaw is 1.5 mm. As the curve deepens, there is a decrease in space in the area of the upper incisors, which leads to their deformation. With a reverse curve, there is a large amount of free space.
Where is the torque lost?
An arc that has the same size as the groove is called full-slot. Arches used for orthodontic treatment using the passive self-ligation technique are always smaller than the slot size, i.e. not full-slotted. Full-slot arches are not used in practice for two reasons. The first is the large forces produced by a full-slot arch. The second is the high resistance to sliding of the arc in the groove as a result of the coincidence of the dimensions of the groove and the arc. Accordingly, the arc always has some freedom of movement and can “play” in the groove. This “play” of the arc in the groove is called geometric loss of torque.
In the Damon system, the play of an arc with a section size of .019 × .025 in a groove with a size of .022 × .028 is 10.5 ° in one direction (according to the manufacturer). The arc cross-section size .019×.025 is the maximum for the passive self-ligation technique and the smaller the arc cross-section size, the greater will be the play of the arc in the groove and, accordingly, the greater the loss of torque.
There is also force loss of torque, where the arc may not have enough force to create a torque even after overcoming the geometric loss. However, there are currently no clear data on the magnitude of power loss.
Thus, it must be understood that when working with the passive self-ligation technique, the torque embedded in the bracket groove will not be fully realized automatically.
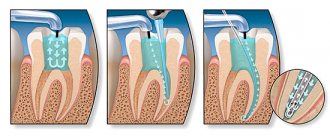
Example. The figure shows that when a tooth is in an abnormal position, for example, with a high torque (1) and a bracket with a standard torque is glued to it, the rectangular arch presses on the walls of the bracket groove, as a result of which the tooth begins to align towards the normal torque and stops 10.5° before its correct position (2). If an additional force is applied to the tooth (for example, an elastic chain), the tooth will move until the arch begins to press with its edges on the walls of the bracket groove, and this position will differ from the normal position of the tooth by 10.5° from its correct position (but in the direction of low torque) (3).
Why do we need torque options in brackets?
Real torque = nominal torque (specified by the manufacturer) ± torque loss.
This equation will only be valid if two conditions are met:
- the difference between the inclination of the tooth after the alignment of the dentition is completed and the torque included in the bracket must be greater than the value of the geometric loss. If this condition is not met, the tooth torque value will not change at all after the alignment phase.
- there is no power loss of torque, i.e. the arc has enough rigidity to create the required amount of torque to change the inclination of the tooth.
You can compensate for the loss of torque in the following ways:
- applying compensating bends to the working arc. This method entails a lot of time and labor, and the quality of the applied bend greatly depends on the skill of the doctor;
- use an additional torque device (for example, a torque spring);
- choosing the most suitable bracket torque option.
The choice of torque is the introduction of hyper-correction for current loss. The grooves of braces with different torques will differ in the angle of inclination of the groove to the base of the bracket. High torque will have a higher value (ie upward) relative to the standard value, and low torque will have a lower value (ie downward) relative to the standard value. High torque will have a higher value relative to the standard value, and low torque will have a lower value relative to the standard value.
There are three torque options in the Damon system:
Example. A low torque bracket is glued to a tooth with positive torque and an archwire of size .019×.025 is installed. The arc twists and with its edges presses on the walls of the bracket groove (1). The tooth begins to move and stops at normal torque. But the tooth did not reach 10.5° to the nominal current value (2). If a full-slot archwire .022×.028 (3) had been used and the nominal torque had been realized, the tooth would have acquired a negative torque (went into retrusion).
Inadequate diagnosis of multifactorial dentoalveolar anomalies often leads to the choice of incorrect treatment tactics, resulting in unstable occlusion. Diagnostics in orthodontics is of great importance, since an orthodontic diagnosis is usually a combination of several anomalies. A small, at first glance, deviation from the norm entails further changes in the closure of the teeth. Thus, any anomaly of occlusion is a symptom complex of several anomalies of the teeth, dentition and jaws, considered in three mutually perpendicular planes.
The goal of orthodontic treatment is static and functional occlusion. One of the main conditions for achieving the six keys of normal occlusion according to Andrews is the proportionality of the jaw bones to each other. Orthodontists use a huge number of cephalometric analyzes to diagnose skeletal and dento-alveolar disorders in the sagittal plane and pay insufficient attention to the analysis of direct teleroentgenograms (DRG), which gives the concept of transversal disorders. When there is a mismatch in the size of the jaw bones in the sagittal plane, the dentition tries to “compensate” by creating occlusal contacts, as a result of which we observe protrusion or retrusion of the incisors. In the transversal plane, due to changes in the width of the nasomaxillary complex, teeth erupt crosswise or change inclination to “avoid” cross-occlusion. This compensation is typically manifested by lingual inclination of the lower molars and premolars, and vestibular inclination of the upper (Fig. 1).
Rice. 1. Negative inclination of molars indicating the angle of their lingual inclination.
The relationship between transversal disorders and functional occlusion
The compensatory changes in teeth in the transversal plane described above are graphically depicted in the literature in the form of a Wilson curve. Thus, excessive inclination of the molars of the upper jaw to compensate for the deficit in the width of the upper jaw is manifested by a pronounced Wilson curve, i.e., the palatal cusps are located below the buccal cusps (Fig. 2).
Rice. 2. In-depth Wilson curve. The buccal cusps are located above the palatal cusps, the “sagging cusps.”
Many articles describe the negative impact of the discrepancy between the CO (central occlusion) and the CR (central jaw relation) on the sagittal and vertical parameters of the dentofacial system. It is described in the literature that “sagging” palatal tuberosities form premature contacts when the teeth are closed, thereby provoking a vertical displacement of the articular process. In the case of premature contacts on the last molars, the patient is forced to move the lower jaw to ensure occlusion. A common symptom in patients with anomalies of occlusion (narrowing of the upper jaw) is the location of the palatal cusps of the lateral teeth of the upper jaw below the occlusal plane, as well as dentoalveolar compensation, expressed by the inclination of the upper lateral teeth vestibularly. Thus, in the absence of cross-occlusion, sagging buccal cusps and a pronounced Wilson curve become the starting point for vertical displacement of the articular process to achieve maximum fissure-tubercle contacts. Moreover, normalization of skeletal abnormalities along the transversal, flattening of the Wilson curve, coordination of the dental arches are an important component for eliminating the discrepancy between the CO and the CO.
The relationship between transversal disorders and periodontal condition
A large number of studies prove that there is a high risk of gingival recession in orthodontic patients if dentoalveolar compensation is attempted for the narrowing of the maxilla. According to the literature, the limit of changes in the size of the dentition in the transversal direction is much less than in the sagittal direction, since due to compression of the thin layer of cortical bone of the alveoli on the vestibular side, minor movements of the teeth can lead to fenestration, loss of bone tissue, and thinning of the gingival tissues. Elimination of premature contacts on the working and balancing sides has also been shown to improve the patient's periodontal status (Fig. 3).
Rice. 3. Recession after orthodontic treatment due to transversal discrepancy in the size of the jaws (lack of cortical bone on the vestibular side of the upper molar) (a) and discrepancy in the size of the dentition in the transversal direction (b).
Diagnostic methods in the transversal plane
In case of changes in the size of the upper jaw along the transverse, the temporomandibular joint (TMJ), periodontal tissue and airways are most susceptible to negative influence. To identify disorders, diagnosis is necessary in all three (sagittal, vertical, transversal) planes. This paper describes some methods for diagnosing transversal anomalies of the dentofacial system, which, in our opinion, need to be included in the examination protocol for orthodontic patients. Regardless of the diagnostic method preferred by the doctor, he should focus on the following criteria for a normal ratio in the transversal plane:
- teeth are located in the center of the alveolar process;
- teeth are aligned in the alveolar process;
— the teeth are in correct contact with the antagonist (Fig. 4).
Rice. 4. The location of the molars in the middle of the alveolar process.
This is important for:
— stability;
- functions;
- TMJ health;
- periodontal disease.
Transversal diagnostics as an integral part of achieving functional occlusion
Traditionally, in orthodontic diagnostics, more attention is paid to measurements in the sagittal and vertical planes. However, the correct definition of transversal parameters is no less, if not more important and informative. Research proves that occlusal interference due to an inadequate Wilson curve plays a decisive role in discrepancies between the CO and the CO, thereby having the most negative impact on periodontal health and craniofacial development.
Analysis by Andrews
In 1970, Andrews described 6 keys of normal static occlusion. Subsequently, Andrews et al. developed a 6-element philosophy for optimal diagnosis. One important diagnostic criterion is Element III of the Andrews philosophy. Element III WALA ridge (Will Andrews and Larry Andrews) is based on the fact that the width of the mandible is determined by the marginal ridge. According to Andrews' definition, the marginal ridge is determined by the most protruding part of the alveolar process on the vestibular side. The WALA ridge coincides with the mucogingival junction at the center of resistance of the mandibular molars. In non-growing patients, the width of the lower jaw and alveolar process, and accordingly the WALA ridge, do not change during orthodontic treatment. Thus, WALA ridge is a stable basis of Element III of the Andrews philosophy (Fig. 5).
Rice. 5. Borders of WALA ridge: front view (a) and view from the occlusal surface (b).
Element III assumes that the upper and lower molars should be located in the center of the alveolar bone, have correct inclination and adequately occlude with the antagonists, i.e., the supporting cusps of the upper molars are located in the fissure of the antagonist teeth. To determine the discrepancy between the upper and lower jaw along the transversal, a certain algorithm is used.
Step 1
The width of the lower jaw or the horizontal distance from WALA ridge on the right to WALA ridge on the left is determined.
According to Andrews' research, optimally positioned mandibular molars should be aligned in the alveolar ridge such that the FA-facial axis point, or crown center, is 2 mm behind the WALA ridge. Based on the above, the width of the lower dentition is determined by the formula:
(WALA ridge on the right – WALA ridge on the left) – 4 mm.
Step 2
The width of the upper dentition depends on the optimal inclination of the upper molars. To determine this width, it is necessary to measure the distance from the FA point on the right molar to the FA point on the left molar. Then evaluate the existing inclination of the upper molars and determine the distance that will appear between the FA points on the right and left when the molars are optimally aligned, using the formula: 1 mm = 5° change in inclination.
The difference obtained in millimeters is subtracted from the original parameter FA on the right and FA on the left. The final result represents the existing width of the maxilla. In order for the molars of the upper and lower jaw to have an optimal transverse relationship with each other, the width of the upper jaw should be 5 mm greater than the width of the lower jaw.
All of the above is clearly demonstrated in the following clinical example:
Lower jaw:
WALA ridge left – WALA ridge right = 50 mm (Fig. 6).
Rice. 6. Width in the WALA ridge area.
FA right – FA left = 44 mm (Fig. 7).
Rice. 7. Width in the FA-FA area.
Accordingly, according to the formula (50 - 4 mm), the FA-FA distance should be 46 mm, i.e. 2 mm more than the existing one (46 - 44).
Conclusion: it is necessary to align the lower molars by 1 mm on each side (change the inclination by adding 5° of vestibular coronal torque to the lower molars).
Upper jaw:
The optimal width of the upper jaw is 46 + 5 = 51 mm.
Initial distance FA left – FA right = 45 mm.
According to direct TRG, the inclination of 16, 26 is increased by 5° on each side, i.e., when the axial position of the upper molars is normalized, the FA point on the right and left will shift orally by 1 mm. Therefore, true FA right – FA left = 45 – 2 = 43 mm. Thus, we need to expand the upper jaw by 8 mm.
CBCT Analysis
Today, CBCT is one of the most dynamically developing three-dimensional diagnostic tools in orthodontics. With the help of CBCT, orthodontists are able to accurately measure any parameters without any distortion. In this regard, in our opinion, the use of CBCT for diagnosing transversal measurements of the skeletal structures of the jaws is very promising. The Ricketts and Andrews methods for quantifying skeletal discrepancies are based on the use of specific anatomical landmarks—the width of the maxilla and mandible. So in Ricketts' analysis these are the points Mx-Mx for the upper jaw and Ag-Ag for the lower jaw.
The Andrews analysis uses the WALA ridge and FA as anatomical landmarks. The WALA ridge measurement on the left and right represents the width of the lower jaw, and the FA measurement on the right and left (using the method described above) determines the width of the upper jaw. Although both of these methods are invaluable for orthodontic diagnosis, the use of CBCT significantly differentiates the identification of anatomical landmarks, thereby minimizing the possibility of error.
As identifying measuring points for the upper jaw, the most optimal point will be point M from the Ricketts analysis, and for the lower jaw, the point from the WALA ridge analysis is taken, since these points correspond to the absolute minimum width of each jaw.
Computer analysis algorithm
1. Open the multiplanar view to simultaneously display sagittal, coronal and axial slices (Fig. 8).
Rice. 8. Multiplanar view.
2. To determine the width of the lower jaw, scroll down the image to determine the furcation of the first molars. Then we scroll the image until the center of the lower molars is identified on the coronal scan (Fig. 9).
Rice. 9. Determination of the width of the lower jaw.
3. Turn on the full-screen axial view and, using the measurement lines as guides, measure the lower jaw until the intersection of the reference lines from the most protruding point of the cortical plate on the right and left (Fig. 10).
Rice. 10. Measuring the width of the lower jaw.
4. For the upper jaw, a similar method is used with the only difference being that the measurements of the Mx point are determined on the axial and coronal reformates, as in the Ricketts analysis (Fig. 11).
Rice. 11. Measuring the width of the upper jaw.
5. Analysis of the width of the upper and lower jaws is carried out at the level of the first molars. By subtracting the width of the upper jaw from the width of the lower jaw, we determine the difference between the two jaws. Both the Ricketts and Andrews analyzes demonstrate that the optimal jaw difference is 5 mm in adult patients. Preliminary analysis with molars aligned in the alveolar process, located at its center, with good intercuspidation, showed a constant difference in jaw width of 5 mm. Previous Penn CBCT analysis showed the same ideal result of 5 mm. To determine the degree of expansion of the jaws for their ideal relationship, it is necessary to subtract 5 mm from the jaw difference. Thus, one of the main conditions for achieving stable and functional occlusion is the correct inclination of the molars, their location in the middle of the alveolar process and the correspondence of the width of the dentition to each other, which will allow to achieve good fissure-tubercle contact of the antagonist teeth and avoid the negative impact of orthodontic treatment on the TMJ and periodontal tissue.
Approximate logic when choosing torque
| LOW TORQUE Recommended for the treatment of non-extraction cases with crowding and/or narrowed dentition (regardless of class), as well as protrusion or protrusion of teeth | HIGH TORQUE Recommended in cases of tremors, extraction or distalization of anterior teeth, as well as in cases of retrusion or tendency to retrusion of teeth |
STANDARD TORQUE Dr. Dwight Damon suggests using standard torque in cases where braces need to be positioned as close to the gum as possible to improve incisor exposure (smile arches), in cases with low occlusal plane angles and severe open bites. Standard torque is also suggested for mandibular anterior teeth in cases with periodontal ligament restriction or damage.
How will the position of the maxillary central incisor change when choosing different torque options?
The graph shows the arc “play” zones in the bracket slot for each torque option in accordance with its color. For Damon braces, this zone is equal to the nominal value of ± 10.5° (rounded to 11 on the graph for convenience).
In other words, in the absence of additional forces, a bracket with a selected torque will not move a tooth located in its “playing” zone of the arch (zone on the graph).
Example 1: if the tooth is in the position of the torque value from +11 to +13, then no bracket will move it, because for any torque option, the arc in this range will be in a passive position and will not interact with the groove. Example 2: High and standard torque brackets will not move a tooth with a torque of +11° to +26° in the absence of additional forces. Example 3: the tooth stands with a high torque and an additional force (spring, chain) acts on it, moving it back. If in this situation a high-torque bracket is glued to the tooth, then the most extreme point at which it will stop is +11°, which is normal. If in this situation you stick a bracket with a standard torque, the tooth will go into retrusion up to +4°.
The most modern Damon prescription system available in Russia is the Damon Q braces system. On the official Ormco website you can read more information about Damon Q braces.
Also, using a convenient bracket picker, you can assemble a set and buy Damon Q online.
№4, 2004
OPPORTUNITIES OF DENTISTRY TODAY
Orthopedic dentistry
A method of taking impressions from the jaws “in a block” without the use of standard or individual trays. Yu.I. Klimashin, A.Yu. Klimashin
The use of immunocorrective drugs in patients using removable dentures. E.G. Pan, A.N. Emelianenko
Best dental clinics Dental training
Therapeutic dentistry
Study of the degree of marginal contact of sealants to dentin of root canals and gutta-percha points during endodontic treatment. Yu.M. Maksimovsky, A.V. Mitronin, L.S. Nekhorosheva
Experience with the use of the drug "Candide" in the treatment of candidiasis of the oral mucosa. THEM. Rabinovich, O.F. Rabinovich, L.N. Gerchikov, M.N. Moiseeva
Study of the influence of ormoker polymerization conditions on its strength. A.G. Ervandyan, R.A. Avetisyan
Disturbances in the functional activity of platelets in patients with chronic generalized periodontitis when combined with diseases of the gastroduodenal region. V.Yu. Shirokov
Toxicity of light-cured composites. D.Yu. Ananikyan
The influence of detoxification therapy using Enterosgel on the duration of remission of chronic generalized periodontitis, when prescribed in combination with the immunocorrector Imudon. Yu.M. Maksimovsky, M.A. Sargsyan, E.V. Volodina
Organization and economics in dentistry Economic activity of a dental clinic in market conditions. L.G. Deineko Clinical and organizational forms of providing therapeutic dental care to the population of a large city at the present stage. Grinin V.M., Polozova I.G.
Optimal directions in solving problems of continuity in the activities of dental specialists. S.A. Zaslavsky, R.S. Zaslavsky
Safety and quality
Certification system for oral hygiene products in Russia. E.B. Sakharov