1231
Malocclusion is an abnormal development of the dentofacial apparatus. It negatively affects chewing ability and causes the development of various diseases and pathologies of the oral cavity. At the same time, patients are more concerned about the aesthetic side of the problem. Crooked teeth make your smile unattractive.
Among the existing methods of treating deviations from the normal development of the dental system during the period of mixed and permanent dentition, orthodontists distinguish the hardware method using orthodontic devices and systems of various designs.
General overview
Despite the high development of dentistry today, bite correction is a number of complex and diverse tasks, the solution of which requires a set of measures and the involvement of specialized specialists.
In some cases, when a doctor encounters a pronounced anomaly or a combination of several disorders at once, treatment takes more than one year before the patient gains straight teeth, the ability to chew food fully and correctly, and smile widely and openly.
Hardware treatment in orthodontics is of particular importance in childhood (from 6 years of age). Various corrective structures are used to eliminate certain problems, they can be supplemented with auxiliary parts with a specific purpose (changing the width of the palate, the shape of the jaw bones, etc.), but they always have the same basic (main) elements:
- basis;
- fixation elements;
- active parts.
In general, treatment with devices is based on the fact that a mechanical effect is exerted on individual teeth and elements of the dentoalveolar system , due to which the restructuring of bone tissue occurs.
External mechanical force works to gradually dissolve old bone and form new tissue cells. The displacement of the elements of the series in the correct direction is accompanied by phonological regeneration of the alveolar process.
A successful shift (reversal) of problem units is ensured by:
- pressure applied to the bone element of the jaw arch, which requires movement in the optimal direction;
- unshakable fixation of the structure and the presence of strong supports;
- sufficient space in the jaw arch to change the position of crooked units;
- absence of obstacles to movement, etc.
Hardware correction consists of two stages - active treatment and retention. At the main stage of treatment, the mechanical parts of the device are activated or its functionally guiding parts are corrected. At the stage of consolidating the achieved results, the device acts passively.
What problems does an orthodontist solve, and at what age can a child’s bite be corrected, according to experts.
Come here if you are interested in when orthodontic tooth extraction is justified.
At this address https://orto-info.ru/ortodonticheskoe-lechenie/osnovnoy-period/distalizatsii-molyarov.html we will consider a device for distalization of molars.
About springs
These devices are mainly installed to speed up the process of expanding or narrowing the gap between units. Dentists distinguish between two types of springs: opening and closing. This classification indicates the function of the spring. The first type of product helps to move teeth apart, the second model helps to reduce the distance between units. The operating principle of the spring is similar to the operating algorithm of the elastomer ligature.
Models that increase the distance between teeth work on the principle of compression. The flat end is pressed into the bracket system and puts pressure on the structure. In turn, the bracket lock presses on the tooth, moving it in the desired direction and freeing up space in the row. Quite often such devices have no alternative, since elastomeric ligatures do not work in the direction of compression.
Closing springs work in reverse order. Special clasps (eyes) are placed on the hooks located in the area of the support tubes, which move the teeth, reducing the distance between the units in the row.
Nickel-titanium alloy is most often used to make springs. This material is reliable, durable and hypoallergenic.
Important! In addition to increased elasticity, the titanium and nickel alloy is able to remember its shape, which helps speed up the treatment process.
The ultra-thin wire, despite its thickness of no more than 0.3 mm, is capable of creating pressure equivalent to a load of up to 200 g. This is enough to displace an incorrectly positioned tooth. An advantage is the possibility of decompression load on periodontal tissues, which prevents the development of mucosal necrosis in the area of impact on the element.
Device classification
Before choosing the type of construction for a specific clinical case, the doctor must assess the general health of the patient’s body, take into account the development of the dental system in accordance with age, the number of teeth that have erupted, and the condition of the periodontal tissues.
Poor installation and fixation of the device in the oral cavity leads to its displacement during therapeutic correction , which prolongs the period of correction and provokes the development of a bad habit of ensuring the stability of the structure in the mouth with the tongue.
Experts divide the entire range of structures for orthodontic treatment into categories:
- directed purpose - preventive, therapeutic, retention (holding);
- technical ability - functional, mechanical, functional-guiding, combined operating principle;
- fastening technique – removable, non-removable, partially removable devices;
- location - extraoral, intraoral on one or both jaws, combined.
If the support fragments are incorrectly selected, various complications can arise, including unwanted movement of the supports under the action of reactive pressure (recoil force). Therefore, the dentist must take the process responsibly.
How are they different from elastomers?
The advantages of springs over these devices are obvious:
- able to move and move teeth apart;
- the constancy of the pressure force accelerates the process of orthodontic treatment (elastomers are only able to provide the required load on the dentition in the first stages of correction);
- biocompatibility of materials with mucosal tissues and tooth enamel.
An important advantage of using springs is the possibility of installing the device at any stage of corrective treatment.
Indications and contraindications
Various designs of orthodontic devices can successfully treat most dental pathologies and dental development disorders. Therefore, orthodontists often give preference to the hardware method of treatment in the following clinics:
- anomalies in the number, shape, structure, position of teeth;
- violation of the deadlines for the eruption of units;
- pathologies of jaw development, disturbance of their growth and structure, deformation, incorrect position in the skull;
- combined anomalies of row elements and jaw bones.
All of the above deviations from the normal state can manifest themselves in the form of deformation of the dentition, malocclusion in various directions.
Orthodontic appliances effectively correct deep, open, cross, prognathic, progenic bites, as well as violations of the basic functions of the dental system, accompanied by cosmetic defects.
Contraindications to treatment are pronounced and congenital anomalies that require preliminary surgical intervention, as well as severe concomitant diseases (for example, oncology, epilepsy, etc.)
Inflammatory processes in teeth and periodontal tissues are considered a temporary limitation for installation.
TYPES OF FORCES OF ORTHODONTIC APPLIANCES
⇐ PreviousPage 4 of 4
Orthodontic forces are usually classified according to the following basic principles: 1. magnitude of impact: weak, moderate, large and very large 2. time of impact: continuous and intermittent 3. nature (principle) of impact: mechanical and functional 4. direction: active (acting on moved area) and reactive (acting on the fulcrum) For the first time, A.M. systematized orthodontic forces according to the magnitude of the impact. Schwartz based on clinical and experimental studies. The calculations are based on the value of intracapillary pressure - 26 g/cm2. So, to the first group A.M. Schwartz attributed small forces - 3-5 g/cm2 - these forces are small and do not cause a periodontal reaction. The second group of forces includes forces less than or equal to intracapillary pressure - 15 - 20 g/cm2. When such forces are applied, microcirculatory blood circulation in the area of the pressure zone is suppressed, which is accompanied by reversible changes in the wall of the alveoli and the root of the tooth being moved. The third group includes forces of 30-40 g/cm2. They suppress blood circulation, which is accompanied by tissue hypoxia and pronounced reversible reactive changes. The fourth group includes large forces - more than 60 g/cm2; they destroy soft tissue by crushing, that is, such phenomena are irreversible after the force ceases. Thus, the optimal force is the second degree.
HAND SPRING AND CURL SPRING
The Kalvelis arm spring is used for mesiodistal movement of teeth and operates on the principle of a serpentine spring. It consists of a free end, two semicircular bends and a process. To make a spring, take a piece of wire with a diameter of 0.5-0.6 mm and a length of 40-50 mm. First, semicircular bends are made, the first of which should be slightly larger than the second. Then the free end of the spring is fitted to the tooth being moved and the process is bent. To prevent the spring from sliding off the tooth being moved, a ring is attached to it, to which the hook is soldered. In addition, in the base of the device, you can strengthen a guide made of wire with a diameter of 0.7-0.8 mm, which prevents the end of the spring from sliding to the cutting edge of the tooth. The coil spring is designed for mesiodistal tooth movement. In some cases, it is used for the purpose of dentoalveolar lengthening or shortening, as well as vestibular movement of the incisors. It consists of three parts: 1) a free end, which serves to transfer pressure to the tooth being moved; 2) a curl, which is an active part of the spring; 3) a process for fixation in the base of the device. The spring is bent from a piece of wire with a diameter of 0.5-0.6 mm and a length of 25-35 mm. It must meet the following requirements: 1) the curl must be directed in the direction opposite to the direction of tooth movement, and located in accordance with the location of the tooth movement; 2) the free end of the spring should end at the transition point of the lateral surface of the tooth crown into the vestibular one and should be located closer to the mucous membrane of the alveolar process. The spring acts as a result of the unwinding of the curl. To do this, it is first activated. The curl should be positioned so as to maximize the translational action of the spring on the tooth being moved and avoid the consequences of its rotational action. If the free end of the spring is located on the vestibular surface of the tooth, then its rotation along the axis and displacement in the palatal or lingual direction are possible.
CLAMP FOR HOLDING ORTHODONTIC APPLIANCES
The reliability of fixation of the orthodontic apparatus using clasps depends on the area of contact of the clasp arm with the tooth crown and its position in relation to the equator. Clasps with a plane touch of the shoulder to the tooth crown, clasps with a linear touch and clasps with a point touch can be used. Compared to the designs of clasps of the first and second groups, clasps of the third group minimally injure the tooth enamel, since they touch it pointwise. They reliably fix removable structures of orthodontic appliances. The most widely used of this group are the Adams clasp and the arrow-shaped Schwartz clasp (Fig. 18).
Rice. 18. Orthodontic clasps: a) Adams clasp, b) Schwartz clasp
VESTIBULAR ARCS
Vestibular arches are used both to correct the position of individual or groups of teeth, and as fixing elements.
A regular vestibular arch can serve as a fixing element and be used to change the inclination of the frontal teeth (moves them in the oral direction) and to delay the growth of the frontal portion of the jaw. There are several types of vestibular arches.
Vestibular arch with a pressure loop (horizontal or vertical on one of the teeth) - used for the vestibular location of one of the front teeth.
Multi-link vestibular arch - used for more corpus movement of the front teeth in the oral direction.
A vestibular arch with M-shaped bends in the canine area is used to correct a vestibular arch located canine, provided there is space in the dental arch. A vestibular arch with M-shaped bends in the middle is used to treat diastema.
A vestibular arch with one semicircular bend is used for lateral movement of incisors, elimination of asymmetrical diastema (which is caused by the incorrect location of one of the incisors), movement of the lateral incisor to the place of the removed central one, for distal movement of canines or premolars. The free end of the arch ends in a hook that encircles the tooth to be moved.
⇐ Previous4
Recommended pages:
Use the site search:
Fixed types
Fixed structures include devices that are fixed in the patient’s mouth once and are not removed until the end of treatment. The period of correction with such devices is usually short, and the retention period is long.
Engla
Universal device. It may have three principles of action depending on its purpose:
- springy – works to expand the dental arches in the chewing areas;
- stationary – removes units from an anomalous position;
- sliding – eliminates protrusion of units of the anterior section.
The device includes:
- crowns, rings for permanent sixes and sevens;
- tubes soldered to rings and crowns on the horizontal side;
- a metal wire arc-shaped element with nuts screwed onto the ends.
To attach crowns and bandage elements, dental units do not need to be prepared.
Derischweiler
Components and parts:
- rings and crowns for a group of units located in the zone of maximum narrowing of the maxillary arch of the upper jaw;
- wire reinforcement soldered to the bandage parts (the tips are welded into the base);
- an expanding helical element connected to the arch and fixed along the midline of the palate.
Operating principle:
- activation of the helical element until slight pain appears in the area of the palatine sulcus (carried out once every three days);
- the screw acts on dental units through the base, alveolar part, arcuate element and crowns;
- within 20 days, the upper jaw expands, the median palatal sulcus opens, which manifests itself in the form of the formation of an interdental gap.
The retention period after correction lasts at least six months. The formed gap is eliminated by moving the central teeth in the medial direction.
Before installing this appliance, it is important to evaluate the depth of coverage of the lower central teeth with the upper ones, since due to the expansion of the dental arch it becomes smaller. If the incisal overlap is weakly expressed, during the movement there is a risk of vertical separation of the dentition.
In addition, the device is not recommended for use if the palate is flat and shallow, since the clinical picture may worsen during correction.
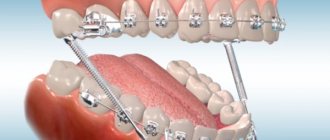
Edgewise technique
All designs of the edgewise technique (advanced Angle technique) include a wire arch (initial, intermediate, final) and braces. Using an arc, you can obtain forces of different directions, which will ensure the displacement of problem elements in several mutually perpendicular planes at once.
In fact, this technique has an important feature - the basis of the apparatus is the arch , and the braces only transfer the pressure it creates to the teeth. In the absence of a wire element, braces can only be used as hooks for ligatures.
The braces are fixed using rings.
When is it prescribed?
Quite often, dentists are faced with the problem of sparse teeth or crowded teeth in patients. It is to solve such problems that springs are most often used.
The part is installed if:
- it is necessary to free up space in the row for new units that are being cut through;
- it is necessary to expand the row for deployed units that have no place in the jaw row;
- Tremas and diastemas were diagnosed;
- there is an artificially created defect (more often it occurs after tooth extraction for medical reasons or its mechanical damage and the impossibility of restoration).
The doctor will prescribe the installation of an additional device if it is necessary to normalize the arrangement of units of the dentition before starting prosthetics, or if there is a need to move the teeth in a row over a considerable distance. In this case, the direction of movement does not matter.
Dentists consider the inappropriateness of use as a contraindication for use in cases where elastomers can be installed or a positive allergy test for metal.
The main reason for patients’ refusal to install springs is the unaesthetic and noticeable element in the oral cavity.
Preparatory stage, installation, timing
| Click to sign up for a FREE consultation |
The advantage of using springs is the ease of installation and dismantling without preliminary preparations. To stretch, the dentist simply places the eyelets on the hooks located in the bracket supports, and the expanders are placed directly on the arches.
Typically, correction with springs lasts from 12 to 18 months. The timing largely depends on the clinical parameters and age of the patient.
Removable structures
The patient wears removable orthodontic structures for a certain number of hours a day. A temporary wearing plan is developed by a doctor.
The main advantage of such systems is that they give the bite the correct direction at the earliest stages of its formation.
The adaptation phase is quite long - on average 14 days, but caring for the device is not difficult.
Plate with vestibular arch
In clinical practice, it is used for oral displacement (shift, rotation) of anterior teeth. A retraction arch can also be used to improve the quality of device fixation.
The arc can be of various configurations:
- classic (standard);
- semicircular;
- L-shaped (effective for moving fangs in the distal direction);
- M-shaped (corrects incorrect position of fangs, often vestibular).
Additional bends on the arc of the plate fix the intermaxillary traction.
With protracting springs
The plate moves in the vestibular direction one or more elements of the frontal section, standing in the jaw arch in the palatal position. The pressure force of the spring part depends on the number of bends :
- odd number – the pressure vector per unit is translational-rotational;
- if the number is even, the translational pressure vector predominates due to the balancing of rotational forces.
To separate the bite, the system is supplemented with platforms.
With arm springs
Used by specialists to effectively shift crooked fragments in the mesiodistal direction:
- eliminating wide cracks;
- distal movement of the three to the place of the missing six (after its removal).
Spring components:
- large and small semicircular bends;
- free tip;
- shoot.
With spring lever
Corrects the position of dental units. The spring is activated after unwinding a kind of pin clamp - a curl. The curled part is directed in the opposite direction of the specified movement.
With orthodontic lock
Works both to lengthen and widen the jaw arches. Placing the plate for expansion requires creating elevations with occlusal pads on the lateral units.
The purpose of the system depends on the position of the screw in the structure:
- parallel to the seam – lengthening effect;
- perpendicular to the middle seam - a symmetrical increase in width.
In the video, a specialist will talk about the use of removable plate devices.
Serpentine spring or pusher
Designed for vestibular movement of teeth. The movement can be body-based or with rotation around an axis. This depends on the design features of the serpentine spring manufacturing. With an unequal number of bends (Fig. on the left), which are located in mutually opposite directions, translational and rotational movements occur, with the same number (Fig. on the right) - only translational, since the forces that act rotationally are balanced.
The force that the spring develops depends on its length, the diameter of the orthodontic wire, the number of bends and their width, as well as the elastic properties of the orthodontic wire. With an increase in the diameter of the wire and a decrease in the length of the acting arm or bending radius, the spring force increases. Most often, springs with two semicircular bends are used. Making springs with more than three bends is impractical, since the active part of the spring becomes long, elastic, easily slides off the moving teeth and interferes with the movements of the tongue.
Functional guides
Functionally, guide devices are systems of intermaxillary action. Such systems allow you to rebuild the myostatic reflex, maintain or, conversely, stimulate excessive development (growth) of the jaw.
Such devices are widely used in orthodontic practice due to their simplicity and effectiveness.
Schwartz Kappa
Used in the treatment of mesial occlusion and retrusion of the anterior units of the upper jaw.
Main features:
- made on six front elements of the movable jaw;
- completely covers the crowns to the marginal gum line;
- the cutting edges are continued by an inclined plane, the height of which is adjusted and adjusted in the oral cavity.
Plate with bite pads
Manufactured for the upper jaw row. Effective in the treatment of deep bite, provided that there is no crowding in the anterior part of the movable jaw.
In what cases is an orthodontist consultation required for children, and what happens in the specialist’s office.
This publication is all about diet while wearing braces.
Here https://orto-info.ru/ortodonticheskoe-lechenie/osnovnoy-period/zubnyie-shhetki-dlya-breketov.html all about how to choose the right toothbrushes for braces.
Functional
The mechanism of action of such structures differs from classical removable devices. They act on the dental system not due to springs and screws, but due to the contraction of the muscular structures of the maxillofacial area.
Kerbitz plate
The design is used for:
- eliminating bad habits in children;
- restoration of breathing through the nose;
- increasing the tone of the orbicularis oris muscle;
- stimulation of the growth of the movable jaw, if the bite is deep or distal, and the frontal units of the movable jaw are tilted in the vestibular direction.
Kraus record
Effectively eliminates frontal disocclusion. Helps cope with the consequences of distal bite and bad childhood habits.
This design differs from the previous device by the presence of a barrier.
Schonherr plate
The plate is equipped with a cutting projection. In orthodontics it is used to eliminate bad habits , resume proper nasal breathing, and stimulate the facial muscles. Promotes the development of the lower jaw.
Contraindication for use is deep occlusion.
Combined action
These devices include active and passive structural parts. Installed to get rid of morphological and functional disorders.
Bruckle apparatus
The system of corrective elements includes:
- plate on the movable jaw;
- inclined plane;
- steel arc;
- clasps on side units.
The device corrects deep bites quite quickly and in a targeted manner.
Basharova's apparatus
The device is a plate (upper/lower jaw) with an active arch and an inclined plane. The system also includes screws and spring elements that act on important points.
Orthodontists prescribe a corrective product if it is necessary to correct a sigital malocclusion.
Activators and bionators
Bionators are devices that can be used to rearrange the position and inclination of units, change the parameters of the jaw row (width, length), and correct incorrect occlusion.
They can be made in the form of a monoblock or a single-jaw design, and can be used for preventive or therapeutic purposes.
Activators often involve fixation on the lower jaw to stimulate its growth.
Experts identify a number of the most effective bionators and activators. The list is as follows:
- Wunderer activator – correction of mesial occlusion.
- Balters Bionator - block protection of rows from lips, stimulation of full closure, restoration of the normal position of the movable jaw and teeth.
- Janson activator – correction of distal occlusion.
- Open Klammt activator – elimination of malocclusion in the sigital plane.
Oval protraction spring
Or a double-arm pusher is designed to move a group of incisors. The active part is oval bends in the amount of 1 to 3, which are made from orthodontic wire with a diameter of 0.5-0.7 mm. If it is necessary to move the entire group of cutters, the spring is made of wire with a diameter of 0.6-0.7 mm.
A modification of the oval spring is our proposed 8-shaped double-arm protracting spring with a flat (for body movement) or round (for movement with rotation around an axis) head.
The springs are activated by increasing the distance between the bends.