2472
Temporomandibular joint dysfunction is a rather complex condition that can be experienced by people of different ages and health conditions.
A large number of different symptoms, difficulties with chewing and opening the mouth are a serious reason to visit the dentist to determine whether a pathology of the lower jaw joint, such as Costen syndrome, is developing.
Description of the problem
Costen's syndrome was discovered in the thirties of the 20th century. Otolaryngologist D. Kosten compared cases of patients complaining of ear pain due to pathologies in the structure of the jaw system, and came to the conclusion that there is a relationship between these factors.
Pathological occlusion syndrome, as Costen's syndrome is otherwise called, is a functional disorder of the temporomandibular joint.
This pathology affects the cartilage disc, which provides joint mobility in three directions, due to which complete chewing of food is carried out.
An unevenly distributed load between the jaws leads to inflammation of the cartilage disc, which can lead to its degeneration if not treated in a timely manner.
As a result of this phenomenon, there is a decrease or complete loss of mobility of the mandibular joint.
Possible complications
If the patient neglects all the symptoms, suffers pain and delays treatment of Costen's syndrome, functional and physiological changes occur in the temporomandibular joint, salts are deposited in its area, fluid accumulates in the cavity due to inflammation, and the ligamentous apparatus is weakened. A person loses the ability to chew food normally due to pain, and has to eat soft foods. Because of this, the diet becomes quite meager, and problems with the gastrointestinal tract may occur.
In the future, complete immobilization of the jaw joints may occur, up to the inability to open the mouth, and significant deterioration in hearing and vision. The syndrome can indirectly damage other systems and organs.
Reasons for development
Dentists still have not agreed on what can trigger the development of the syndrome.
The most common factors contributing to the development of the disease are the following:
- incorrect design of the denture, causing uneven distribution of load during chewing;
- various jaw injuries;
- congenital or acquired pathological bite;
- excessively strong one-time or constant loads on the jaw joint;
- bruxism;
- collagen diseases.
The development of Costen syndrome can be caused by a combination of several factors or by one of the above reasons.
If you find any problems in the operation of the dentition, you should consult a dentist.
How can a pacifier affect a child’s bite, tips for selection and use.
Read here all the most important things about the small vestibule of the oral cavity.
At this address https://orto-info.ru/zubocheliustnye-anomalii/chelyustey/krivaya-ne-prigovor.html we will talk about methods for correcting a crooked jaw.
Causes of Costen syndrome
To date, the causes of this pathology remain unknown, but gnathologists are similar in their belief that the main prerequisites for the formation of Costen syndrome are:
- uneven load on the jaws when chewing, due to incorrect design of the denture;
- jaw injuries;
- malocclusions of various origins;
- too intense load on the jaw;
- bruxism – grinding of teeth during sleep;
- collagen diseases.
Risk factors
Dentists note that most often the development of Costen syndrome is observed in patients over 50 years of age. As a rule, the likelihood of its occurrence is higher in women than in men.
People who have a history of the following problems also fall into the risk category:
- injuries of the temporomandibular joints;
- unresolved violation of the structure of the dentofacial rows;
- absence of the last molars in each row;
- osteoarthritis.
Some dentists suggest that genetic predisposition can also become a factor in the development of pathology, however, this assumption has not been proven.
Symptoms
Costen's syndrome is characterized by the presence of a collection of symptoms that are rarely interrelated.
In addition, in the initial stages of the disease, symptoms may not appear, which delays the patient’s visit to the dentist and complicates timely diagnosis.
Most often, patients experience the following signs of disease development:
- pathologies in the functioning of the temporomandibular joint - difficulties during opening and closing of the jaw, the appearance of crunching and clicking, severe pain during chewing;
- the appearance of dryness and acute pain in the root of the tongue and pharynx;
- the formation of a herpetic rash on the mucous membranes of the oral cavity and the outer edge of the ear canal;
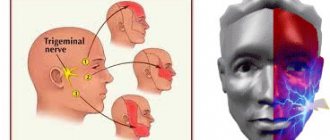
- the occurrence of trigeminal neuralgia - severe pain of a paroxysmal nature that affects one side of the face - jaw, cheek, ear, eye;
- pain in the ears and head, which may worsen when sneezing or singing.
In some cases, patients may experience frequent dizziness, hearing loss, and pain in the cervical spine.
Differential features in the diagnosis of Costen's syndrome with Meniere's disease
Many doctors often call the common disease Costen syndrome a “chameleon disease.” The features of the course of this disease can easily be confused with acute otitis media [1,2,5] or arthritis of the jaw joint. The disease was first described by American otolaryngologist James Kosten, who was able to discover a connection between the pathology of the dental system and acute ear pain in his patients. In 1934, he published an article detailing his accumulated observations. Thus, a new disease appeared in medical reference books, which subsequently received the name of its discoverer [1,3,4]. According to various authors, Costen syndrome occurs in 25–65% of the world's population. The vast majority of them are women; in adolescence and young adulthood, the incidence rate is 16-30%.
The clinical picture of the disease is varied. However, all patients have one common symptom - the inability to open the mouth wide during the three-phalanx test. Patients with Costen's syndrome cannot do this. Even if the disease is not long ago, they can only fit the joints of one or two fingers into their mouths. Complaints of pain in the ears and head, aggravated by chewing, sneezing, singing, pain radiating to adjacent areas of the face and neck, are also a signal symptom [3]. Pinched nerve endings that pass near the jaw joints explain the appearance of pain. Depending on how many joints are affected (one or both at once), the pain can be unilateral or bilateral. Due to the absence of nerve endings in the joints, if their functioning is disrupted, pain in this area is felt in the ears, in the neck, head, as well as in trigger points (seals) of the facial muscles, in these cases pain is felt when pressing on them.
As is known, dysfunction of the temporomandibular joints can be caused by various reasons - malocclusion, high physical activity, stress (nervous experiences provoke persistent spasm of the masticatory muscles), jaw injuries, inaccurate chewing of solid food, excessive opening of the mouth when laughing, yawning, singing. However, the syndrome is often caused by dental errors. For example, when installing an oversized filling, the load on the jaw will begin to be distributed unevenly and can cause corresponding symptoms. A similar problem can arise with unsuccessful prosthetics. Tinnitus and clicking sounds when moving the lower jaw appear already in the later stages of the disease [3,6].
In rare cases, patients may experience: hearing impairment, dizziness, changes in taste sensitivity, bruxism (teeth grinding), back pain, twitching of the eye muscles, eye pain, photophobia.
The purpose of our study was to study the features in the diagnosis of damage to the auditory and vestibular organs in Costaing syndrome and Meniere's disease.
To study this goal, we put forward the following tasks:
- study the components of vestibular ataxia in patients with Costen syndrome;
- study the components of vestibular disorders in patients with Meniere's disease;
‒ develop criteria for the differential diagnosis of Costaing syndrome and Meniere’s disease.
The study was conducted at the Department of Otorhinolaryngology of the Andijan Medical Institute Clinic. There were 13 patients in the study, of which 69% were women (9), men were 31% (4). The average age of the patients was 40.8±3.9. The mean age of women was 42±4.9, and the mean age of men was 37.5±11.3. All patients underwent general clinical examinations of blood, urine, instrumental examinations of the organ of hearing and balance (audiometry, acoustic impedasometry, otoacoustic emission, rotational tests). The results obtained were statistically processed.
Based on the results of the examination, we divided all patients into two groups: in group A there were patients with complaints of severe dysfunction of the vestibular apparatus; in group B there were patients with no such complaints of dysfunction. When analyzing the results obtained, it is clear that dysfunction of the vestibular analyzer in almost all patients manifested itself in the form of dizziness, nausea, vomiting, ocular nystagmus, ataxia and sweating. However, dysfunction of the vestibular analyzer was more pronounced in all forms in the group of patients with Meniere's disease. Among patients in group A, forms of dysfunction were more pronounced in women than in men. In group B, despite the fact that the patients did not complain, the severity of dysfunction of the vestibular apparatus during the examination was also noted to be greater among women.
Table 1
Comparative characteristics of the components of vestibular ataxia
| Signs | Meniere's disease | Costen's syndrome |
| Pain | — | ++ |
| Duration of the disease | Cannot be detected | Can be identified |
| Dizziness | ++; paroxysmal, 1–2 times a year | +; stable |
| Nausea | ++; at the time of the attack | ±; |
| Vomit | ± | — |
| Nystagmus | ++; | — |
| Sweating | +; at the time of the attack | — |
| Hearing loss | +; fluctuating | In late periods of the disease |
| Noise in ears | +; at the time of the attack | +; permanent, on the side of the affected joint |
| Taste sensitivity of the tongue | Fine | There is a decrease |
| Overview R-graphy | — | Change in the h/h joint |
| Balance imbalance | ++ | In late periods of the disease |
Note: + - mild symptoms; ++ - pronounced signs; ± - periodically appearing signs; - absence of a sign
Analysis of the study results, presented in Table 1, showed significant similarity in the manifestation of signs of vestibular ataxia in Meniere's disease and Costen's syndrome. However, with a directed comparison of characteristics, characteristic specificity can still be detected. For example, the ratio of the amplitudes of the total potential to the potential of the auditory nerve in 5 patients was 0.67, which is typical for Meniere’s disease, and in the remaining patients this figure was 0.22. It is important to establish the fact of the presence of endolymphatic hydrops of the labyrinth as a differential diagnosis. Characteristic of hydrops of the labyrinth is an increase in the amplitude of the total potential as the intensity increases with a corresponding increase in the ratio of the amplitudes of the total potential to the potential of the auditory nerve. In a word, during differential diagnosis it is necessary to pay more attention to the presence of signs of endolymphatic hydrops. According to JB Costen, compression of the lymphatic vessels by the posteriorly displaced head of the temporomandibular joint provokes components of vestibular dysfunction, since the possibility of compression of the chorda tympani is not excluded.
During the study, we also carried out a gender analysis of the manifestations of Meniere's disease and Costain's syndrome, the results of which are presented in Table No. 2. From the indications it is clear that the gross incidence rate prevails among women and, in addition, it can be noted that adolescence and middle age in women can be considered an age-related risk factor for the development of the disease and, accordingly, complications.
table 2
Gender analysis of age-related risk factors for developing the disease
| Age (in years) | Quantity | Central age option | ||
| women | men | continuous | note | |
| 16–20 | 2 (1-M; 1-K) | 1 TO | 18 | High risk age |
| 21–30 | 1 TO | 26 | ||
| 31–40 | 1 TO | 36 | ||
| 41–50 | 3 (1-M; 2-K) | 1 TO | 46 | High risk age |
| 51–60 | 3 (2-M; 1-K) | 56 | High risk age | |
| 61–70 | 1M | 66 | ||
| Total | 9 (4-M; 5-K) | 4 (1-M; 3-K) | ||
Note : M - Meniere's disease; K - Costen's syndrome
The indicators in Table No. 2 also indicate that the age risk factor among women and men is laid out in the period from 41 to 60 years.
In conclusion, it should be noted that the main distinguishing criterion of Costaing syndrome from Meniere’s disease is a pain symptom, which is then accompanied by cochleo - vestibular dysfunction. The introduction of a program for monitoring the functional state of the vestibular analyzer will reduce the risk of complications from the vestibular analyzer in patients.
Literature:
- V. I. Babiyak, J. A. Nakatis. Clinical otorhinolaryngology: A guide for doctors / V. I. Babiyak. - St. Petersburg, 2005. - 800 p.
- V. T. Palchun. Otorhinolaryngology: National guidelines / V. T. Palchun. - Moscow, 2008. - 960 p.
- A. A. Timofeev. Maxillofacial surgery: textbook / A. A. Timofeev. - K.: VSI "Medicine", 2010. - 576 p.
- Gavin J. Vestibular function following unilateral cochlear implantation for profound sensorineural hearing loss / Gavin J. le Nobel, Euna Hwang, Adrian Wu, Sharon Cushing and Vincent Y. Lin // Journal of Otolaryngology - Head and Neck Surgery (2016) 45:38 DOI 10.1186/s40463–016–0150–6
- Kim HA Otolith dysfunction in vestibular neuritis / Kim HA, Hong JH, Lee H, Yi HA, Lee SR, Lee SY, Jang BC, Ahn BH, Baloh RW. // Neurology. 2008;70:449–53.8.
- Ward BK Prevalence and impact of bilateral vestibular hypofunction - results from the 2008 US. Ward BK, Agrawal Y, Hoffman HJ, Carey JP, Della Santina CC. // National Health Interview Survey. JAMA. 2013;139(8):803–10.
Classification
During the development process, pathological bite syndrome goes through four stages, each of which is characterized by the following symptoms:
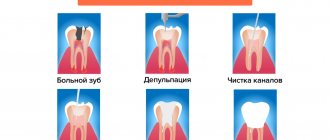
- First stage. The size of the joint space narrows unevenly, and slight loosening of the ligament apparatus is observed. A person begins to experience the first symptoms of a pathological change in the cartilage disc.
- Second stage. The mobility of the temporomandibular joint decreases, ossification occurs in the area of the condylar process of the mandible.
- Third stage. Degeneration of the cartilage disc continues, and sclerosis of the articular surfaces develops. Movement of the lower jaw is severely limited.
- Fourth stage. The patient experiences a strong proliferation of fibrous tissue, and the mobility of the lower jaw is completely absent.
A person experiences persistent pain in the jaw area, radiating to the ear or cheek. At this stage, treatment is carried out exclusively by surgical methods.
TMJ dysfunction - symptoms and treatment
There is no single, universal method for treating TMJ dysfunctions. Full treatment may be hindered by pain that does not allow the necessary therapeutic measures to be carried out.
Conservative therapy allows you to relieve acute manifestations of pathology, ensures the weakening or complete disappearance of symptoms and restores the function of the lower jaw in full.
Physiotherapy is effective in reducing pain. To reduce pain, fluctuarization is used in the TMJ area. The essence of the procedure is the use of alternating, partially or fully rectified low-voltage electric current with a chaotically varying oscillation frequency. Fluctuarization helps reduce pain after 2-3 sessions. If the myogenic nature of the pain is caused by myositis (inflammatory damage to the skeletal muscles) due to contact involvement of the muscle in the inflammatory process, then treatment should first of all be aimed at eliminating the cause of the inflammation.
Amplipulse therapy (sinusoidal modulated current therapy) has shown effectiveness in the treatment of myofascial syndrome (a chronic condition in which pain points form in muscle tissue), reducing the tone of spastically contracted muscles.
Pain of joint origin is treated by prescribing phonophoresis with hydrocortisone, which allows to relieve pain in the acute period and reduce inflammation.
All types of treatment must be carried out under the control of electromyography to assess the effectiveness, equalize and normalize the electrical potentials of the muscles.
During complex treatment, the patient himself must perform myogymnastics after proper training in the technique. It includes passive and active exercises for the moving muscles of the lower jaw and neck muscles. Passive exercises are carried out without load; the patient needs to perform various movements of the lower jaw. Active exercises also include various movements of the lower jaw, but with a load (the patient’s arms counteract the movement being performed) [3]. Exercises should be done 3 times a day for 10-15 minutes.
To normalize bite and occlusal disorders, special orthopedic treatment methods are used - correction of occlusion and the use of orthopedic structures (splints, mouth guards, bite blocks, myostimulation, etc.).
Surgical treatment methods are used for serious morphological pathological changes in the joint. The main indication for surgical treatment is anterior displacement of the intraarticular disc.
Surgical treatment consists of focal chondroplasty of the disc or head of the lower jaw using autologous cartilage (usually nasal cartilage). It is also possible to reduce the disc and suturing the stretched intra-articular ligaments and joint capsule. These methods are aggressive for a complex articular system and they do not always give good results [11].
In the complex issue of treating TMJ dysfunction, over time, the most effective scheme has proven to be the use of medication, manual therapy, physiotherapy and orthopedic treatment aimed at restoring the dentition and normalizing the bite.
Consequences
Lack of treatment in the initial stages of the disease can lead to a significant deterioration of the situation, increased pain and decreased mobility of the temporomandibular joint.
Among the common complications of Costen syndrome, the most common conditions are:
- Indigestion. Due to limited mobility of the jaw joint and severe pain that accompanies the chewing process, grinding hard foods in the oral cavity is noticeably impaired. This entails an increased load on the organs of the gastrointestinal tract.
- Weakening of the ligamentous apparatus. As a result of this phenomenon, a fairly free exit of the head of the lower jaw from the articular fossa occurs.
- Accumulation of inflammatory exudate in the joint cavity. An excessive amount of fluid in the joint cavity contributes to a loose fit of the disc to the head. As a result, popping sounds occur when the jaw moves.
Stages of development and diagnosis
The syndrome does not appear immediately. In its development, it goes through four stages, each of which is characterized by the following pathologies:
- The gap between the joints decreases, the ligaments are slightly weakened.
- The posterior process of the lower jaw, connecting to the temporal bone, ossifies, and the mobility of the joint decreases.
- The cartilage is destroyed, dense connective tissue forms on the surface of the joints, and jaw movements are limited.
- The joint is completely immobilized, the patient constantly experiences severe pain, which analgesics cannot cope with.
The earlier the disease is detected, the easier it is to treat, so you need to consult a doctor in a timely manner. The specialist will diagnose and prescribe appropriate therapy.
Because symptoms are nonspecific and each may indicate a different problem, a comprehensive examination is required to make a diagnosis. The doctor carefully listens to all the patient’s complaints, then conducts a computer and magnetic resonance imaging examination of the joint area, nasopharynx, and paranasal sinuses. The latter method is especially informative, since it allows you to visualize individual elements of the joint without radiation exposure to the body.
Since the temporomandibular joint is connected by ligaments to the malleus of the middle ear, hearing acuity is measured using an audiometer. If the clinical picture is similar to arthrosis or arthritis, panoramic X-rays of the lower jaw are taken. With the syndrome, they should not be affected by pathological changes. In addition, electromyography of the muscular masticatory apparatus and impedance examination of the middle ear may be needed.
Additionally, the doctor can check the smooth sliding of the heads of the jaw joints. To do this, the patient is asked to tightly close the ear canals with his fingers and move his jaw. In the case of Costen's syndrome, characteristic clicking and crunching occurs due to the loose fit of the disc to the articular head.
Sometimes the symptoms described by the patient are very similar to Costen's syndrome, but there is no joint damage. In this case, it is necessary to check the condition of the masticatory muscles. If, with the mouth open, the joints of the middle, ring and index fingers do not pass clearly between the lower and upper incisors, there is a high probability of muscle damage.
If necessary, the doctor carries out other procedures necessary in his opinion, and may also recommend that the patient additionally consult with an otolaryngologist, neurologist, geneticist or orthodontist.
Diagnostics
To determine Costen's syndrome, the dentist must carry out a number of mandatory procedures, since the presence of a variety of symptoms often complicates the diagnosis:
- Examination of the patient and clarification of existing complaints.
- Phalangeal test to detect Costen's syndrome. The essence of the method is that in the absence of disease, during the opening of the oral cavity, the phalanges of three fingers should be located unhindered between the teeth of the opposite jaws.
If this is problematic and only two fingers fit into the gap formed, the dentist concludes that there is temporomandibular joint dysfunction. - Tympanometry of the ear. The examination allows us to identify the presence or absence of middle ear pathologies in order to correctly diagnose the disease.
- An X-ray examination is carried out to determine the condition of the dentition and the structural anomalies present in it.
- Consultation with relevant specialists. To exclude diseases with similar symptoms, an examination by an otolaryngologist, orthodontist, or neurologist may be required.
Indications for compactosteotomy and surgical technique.
In this publication, see photos of tooth protrusion.
Follow the link https://orto-info.ru/zubocheliustnye-anomalii/zubov/kolichestva/skuchennost-i-sposobyi-ustraneniya-problemyi.html if you are interested in methods for treating crowding of the lower row of teeth.
General prevention
In order to never encounter the syndrome, much less its complications, you need to avoid using chewing gum, as well as excessively frequent consumption of solid foods that are difficult to chew. It is also better to give up the habit of clenching your teeth during nervous tension.
It is necessary to solve problems with unhealthy teeth, their partial absence, and malocclusions in a timely manner. This should only be done by qualified personnel. Also, if possible, you should avoid injuries and inflammation of the jaw.
If chewing begins to cause discomfort or other signs of the syndrome appear, you should definitely consult a doctor. The earlier the diagnosis is made, the easier and more successful the treatment will be, and the risk of complications will decrease.
Treatment
After making a diagnosis, the specialist makes a decision on the need for specific therapeutic measures.
Their complexity depends on the severity of the pathology, however, in any case, the patient must follow the following recommendations to help reduce the load on the jaw joint:
- Stick to a diet. It is necessary to stop eating hard foods and switch to soft and pureed foods. It is advisable that the basis of the diet be
cereals, purees, dairy products.
- Avoid prolonged socializing and chewing gum to reduce the impact on the jaw.
- Reduce stress levels in everyday life, since high nervous tension increases pain impulses.
- Sanitate the oral cavity to eliminate problems that may serve as aggravating factors.
Drug therapy
To eliminate the inflammatory process and relieve pain, specialists can prescribe the patient a complex of medications, which includes:
- Painkillers and anti-inflammatory drugs - Ibuprofen, Dexalgin, Brustan, Ketonal. The drugs have a high analgesic effect and reduce the manifestation of the inflammatory-degenerative process in the cartilage disc.
- Activators of metabolism in tissues - injections or Solcoseryl gel, tablets, ointment or Actovegin gel. Thanks to these drugs, the regenerative process is stimulated and tissue trophism is improved.
- Drugs from the muscle relaxant group help reduce the tone and tension of the jaw muscles and reduce the severity of muscle spasms. Most often, experts prescribe drugs such as Baklosan, Sirdalud, Tizanil.
- Multivitamin complexes – Neurodiclovit, Milgamma, Neurobion, Neuromultivit. Due to the high content of B vitamins in these preparations, pain in inflamed joints is relieved, the processes of creation and blood circulation are improved, and the functioning of the central nervous system is stabilized.
- Sedatives - Afobazol, Fabomotizol, Noofen, which reduce feelings of anxiety and tension, making the pain impulse less pronounced.
Physiotherapy
If a disease is detected at the initial stage, a set of physiotherapeutic procedures, which includes the following measures, may be sufficient to eliminate it:
- fluctuarization of the masticatory muscle area - the procedure has a relaxing and analgesic effect;
- electrophoresis of drugs allows you to increase their effectiveness in reducing pain, relaxing muscles and improving regenerative processes;
- diadynamic therapy - exposure to continuous pulsating current for several minutes produces a pronounced anesthetic effect and helps improve tissue trophism;
- UHF therapy , which is a general and local effect of an electric field, allows you to deeply and evenly heat the inflamed tissue, increasing the rate of its regeneration.
To increase the effectiveness of therapy, experts recommend combining physiotherapeutic procedures with massage of the jaw area, myogymnastic exercises, and acupuncture procedures.
In addition, the orthodontist may recommend the use of a special device that limits the degree of opening of the oral cavity, which reduces the load on the joints.
Surgery
The surgical method of eliminating Costen's syndrome is used at an advanced stage of the disease when other methods of therapy are ineffective.
Surgery is risky because there is a risk of severe bleeding, nerve damage, or scarring of the joint.
At the same time, surgery to remove elements of the temporomandibular joint, such as the cartilage disc or head, may be the only option to restore the proper functioning of the jaw.
In this case, in place of the removed elements, the specialist installs a graft, which allows you to restore proper contact and opening of the jaw rows, as well as establish a painless chewing process.
Discussion
The pathology of the TMJ has been the subject of study by dentists, maxillofacial surgeons, neurologists and ENT doctors for many years [8–12]. Within each specialty, as a rule, narrow aspects of the pathogenesis of Costen syndrome and the possibility of their correction are considered. Thus, maxillofacial surgeons restore the correct relationships of the elements of the TMJ, the activities of orthodontists are aimed at restoring adequate occlusal relationships, neurologists use mainly medicinal methods to combat tinnitus, and ENT doctors often identify and treat dysfunction of the auditory tube, which is associated with noise in the ear and dizziness. At the same time, a general idea of the problem that takes into account all components of the disease is not formed, and therefore, treatment results are rarely satisfactory.
The paired TMJ is one of the most complex joints of the human body and includes a special type of head of the jaw bone, the presence of an intra-articular disc and the Pinto ligament connecting the disc to the handle of the malleus, masticatory muscles that have a certain effect on the muscles of the middle ear and muscles that regulate the lumen of the auditory tube. The abundance of options for disruption of these diverse connections gives rise to a wide range of clinical manifestations of TMJ pathology, representing Costen's syndrome. One should also take into account the different adaptation limits of patients: from the absence of clinical symptoms even in the presence of articular pathology to a detailed picture of articular dysfunction when the compensation limit is reached.
The severity of the pain syndrome can increase with the formation of central sensitization due to disruption of the functioning of the central mechanisms of pain perception [13]. This usually occurs along with the development of emotional distress due to chronic pain; the pain syndrome acquires a special character and requires the prescription of antidepressants and/or anxiolytics [14].
It turned out that only a combined effect, including drug therapy, correction of osteopathic dysfunctions and splint therapy, led to a complete clinical effect and stable restoration of intra-articular relationships (n=14; 93%). In the only case of a partial effect of complex therapy, there was an anterior displacement of the heads of the mandibular bone without restoration of the relationships when opening the mouth, combined with pronounced occlusal disorders. Resistance to therapy in this situation was due to the length of the medical history (16 years) and the formation of dystrophic changes in both TMJs.
It should be noted that if drug treatment of pain, myofascial and anxiety-depressive syndromes was carried out within the framework of current recommendations, then the osteopathic component of therapy included a kinesiological assessment of postural disorders with their subsequent correction [15-17]. This approach made it possible to more effectively combat pain and inactivate myofascial trigger points in groups 1 and 3.
Price
The cost of eliminating Costen syndrome depends on the severity of the pathology and treatment methods:
| Procedure name | Cost of carrying out, rub. |
| Fluctuarization | 800—1700 |
| Electrophoresis | 900—2700 |
| Diadynamic therapy | 500—1500 |
| UHF therapy | 600—1500 |
| Acupuncture | 3 000—4 000 |
| Massage | 1 700—3 200 |
| Surgery (arthroplasty) | 55 000—100 000 |
The large difference in prices is explained by the location of the clinic, the professionalism of the staff and the average cost of similar services in different cities of the country.
Additional information about the temporal joint anomaly is presented in the video.