Author of the article:
Soldatova Lyudmila Nikolaevna
Candidate of Medical Sciences, Professor of the Department of Clinical Dentistry of the St. Petersburg Medical and Social Institute, Chief Physician of the Alfa-Dent Dental Clinic, St. Petersburg
Gum disease is one of the most common phenomena in dentistry. The leading places among them are occupied by periodontitis, inflammation of the gum pocket, and loose gums.
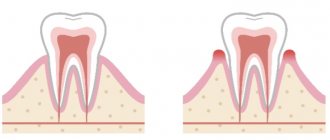
In a healthy state, the gum fits tightly to the tooth. The permissible peeling depth is about three millimeters. This condition is not critical and is even normal; in this case, the pocket easily cleans itself of bacteria and small food particles. It is enough to brush your teeth in a timely manner. However, if the situation develops unfavorably, the pocket expands and becomes deeper. Plaque and food debris accumulate inside, and it becomes impossible to get rid of them with a toothbrush.
Sediments become a breeding ground for bacteria, which provoke further development of the disease.
You should be wary if you notice the following symptoms:
- Bleeding gums;
- Tissue swelling;
- Redness around the teeth;
- Painful sensations when brushing teeth;
- Bad breath;
- Tartar deposits and the appearance of soft plaque.
Formation of a pocket in the gum can lead to serious problems. In later stages, exposure of the necks of the teeth develops. Pathogenic organisms penetrate deep into the tissues, affecting bone tissue and roots, which leads to tooth loss.
Causes of gum pockets
The main reason for gum detachment from a tooth is poor oral hygiene. Incompletely cleaned plaque lingers on the enamel, hardens and forms a stone. This, as well as uncleaned food debris, contributes to the active proliferation of bacteria. They penetrate into the formed hood and gradually lead to an inflammatory process.
Some other factors may also influence the development of the disease:
- Inappropriate hygiene products (too hard toothbrush, aggressive toothpaste);
- Smoking;
- Lack of vitamins;
- Excessive consumption of sweets;
- The presence of certain chronic diseases.
Treatment of gum pocket inflammation
In the early stages and with timely treatment, the disease is easily treatable. You should not try to cure yourself with the help of widely advertised toothpastes or mouth rinses. Only a specialist can prescribe adequate therapy after conducting the necessary research. As a rule, they include:
- Initial examination;
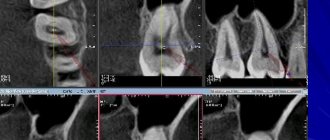
- Taking panoramic x-rays that show all the teeth at once, as well as the depth of tissue damage. This will allow you to choose the right treatment method.
- If necessary, a comprehensive examination for the presence of chronic diseases;
- Making a diagnosis and developing a plan for further action.
As a rule, gum inflammation is treated in several stages. This is a process that requires not only the professionalism of a dental specialist, but also the active participation of the patient himself.
Stage 1. Removing dental plaque
It is plaque and tartar that are sources of bacteria. Therefore, they need to be removed first. This may require several procedures, depending on the extent of the damage to the teeth.
At this stage, special attention is paid to cleaning the gum pockets. It is very important to remove stone and plaque from this area as it is the most difficult to reach at home. In addition, gum pockets “open” the way for bacteria to reach the deep tissues of the tooth.
Stage 2. Anti-inflammatory therapy
This stage is started only when dental plaque is completely removed. The dentist rinses the gum pockets with special antiseptic solutions and applies a gel that relieves inflammation.
In addition, home therapy is prescribed: rinsing with antiseptics and special gels. The patient performs this treatment independently twice a day for the time specified by the doctor.
Stage 3. Recommendations for oral hygiene
Without the patient's compliance with this point, a successfully treated disease may develop again. At this stage, the dentist should tell you which toothbrush and what teeth cleaning products you can use, as well as explain the rules for caring for your teeth.
Brushing your teeth is done with short and gentle rotational movements. Try to reach even hard-to-reach areas. It is convenient to carry out the procedure in the following sequence:
- Cleaning the outside of teeth, both front and back. The top and bottom rows are cleaned separately.
- Cleaning the inside of teeth. Pay special attention to the outermost chewing teeth in the upper and lower rows.
- Cleaning chewing surfaces.
- Cleansing the tongue, including at the root. This is where a huge number of bacteria accumulate, which can easily migrate to the gums and teeth. Plus, cleaning your tongue keeps your breath fresh.
Prevention of gum pocket inflammation
Following simple recommendations will prevent the development of periodontitis and relapses.
Use of specialized therapeutic and prophylactic toothpastes. Due to their special composition, they ensure hygienic cleanliness of teeth and protection of gums from inflammation. Asepta Sensitive toothpaste has this effect. It contains calendula extract and protects teeth well from bacteria. In combination with it, it is recommended to use Asepta gum gel. It contains propolis, known for its healing properties.
Carefully monitor oral hygiene. It's not enough to just brush your teeth. You should also use mouthwash regularly. The Asepta mouthwash has a good effect. It freshens breath, relieves inflammation and pain, and has an antibacterial effect. In addition, it is necessary to use dental floss after each meal to thoroughly clean the interdental space.
Eat more raw apples, carrots, and cucumbers. This food promotes gum massage and natural teeth cleaning.
Regularly undergo preventive examinations at the dentist, at least twice a year.
What parents need to do
- Parents must demonstrate that teeth should be brushed on all sides;
- Move the brush from the gum to the edge of the tooth. For the first teeth, you need to choose a special children's toothpaste and a brush with soft bristles. Teeth cleaning gel is best.
- There is no need to choose toothpaste with excessive fluoride content. While brushing teeth, the child involuntarily swallows the toothpaste, and fluoride can cause irreparable harm to the child’s body.
By the age of 3, children have already mastered the technique of brushing their teeth well, but parents should always be present when brushing their baby’s teeth.
Between the ages of 5 and 12 years, a child's molars begin to erupt. At this time, the enamel on the teeth begins to mature, so you can already use toothpaste containing fluoride.
Parents have the opinion that damaged baby teeth do not need to be treated, because they will fall out anyway. This is an erroneous opinion and caries that appears on baby teeth must be cured.
When do baby teeth appear?
The rudiments of baby teeth appear in the embryo at about 5-7 weeks of pregnancy. By the time a child is born, the crowns of 10 temporary and 8 permanent teeth have already been formed in his jaws. The timing of the eruption of baby teeth is quite arbitrary. The average formula is as follows: the child’s age in months minus 6. That is, the first 2 teeth (usually the lower middle incisors) appear at 6-7 months, the next 2 (upper middle incisors) at 8-9 months. Next, the upper lateral incisors usually come out, then the lower lateral incisors, then the front molars, canines, and back molars. Thus, by the age of 2-2.5 years, the child should have all 20 milk teeth. These are ideal timing and ideal sequence; deviations from them are quite common. Teeth may begin to appear as early as 4 months, or may linger for up to 8-9 months. In rare cases, a baby is born with teeth already erupted.
If your little one doesn’t “meet the deadline,” don’t be alarmed. This does not mean that the child is developmentally delayed. You should also not be proud of the early appearance of teeth - it does not indicate the child’s superpowers. Early or late appearance of teeth may be a hereditary factor. In case of a strong deviation from the schedule - the appearance of teeth before 4 months or their absence after 9 months - just show the baby to the pediatric dentist. In general, the first examination by a pediatric dentist should be scheduled at least when the child is one year old. The doctor will see how the teething process is progressing and talk with you about the baby’s oral hygiene. The baby will get acquainted with the environment of the office, with the doctor, will get the first positive experience of visiting the dentist, because nothing unpleasant awaits him during this visit, and funny pictures on the walls of the clinic, toys, a chair in which he can ride with his mother - all this will certainly have an impact on him. him a good impression. From now on, you should take your child to the pediatric dentist at least twice a year.
Characteristic age-related changes during growth
Eruption of the crown means that it becomes vulnerable to external factors, which include both pathogenic bacteria and mechanical stress. The enamel and dentin layers undergo the first changes - studies show that the height of teeth decreases by an average of 0.035 mm every year, which is caused by the wearing off of the protective coating. A more intense decline is a pathological sign, as well as a consequence of the abuse of bad habits.
With age, the natural shade and structure of the enamel coating changes. Cracks and chips form, coloring pigments accumulate, and areas are formed through which plaque containing pathogenic microorganisms penetrates into the fabric. It is worth noting that the human body does not have a mechanism for regenerating tooth enamel, so any damage requires a medical examination and, if necessary, comprehensive treatment that eliminates negative consequences.
Age-related changes in the pulp
Aging also affects the internal structure of teeth. A reduction in pulp volume, as well as the formation of fibrous deposits, leads to the accumulation of minerals that worsen the condition of the internal vessels and capillaries that provide nutrition to the element. Among patients in the older age group, pulpal atherosclerosis is often diagnosed, which results in fragility and vulnerability of the teeth.
Changes in bone and gum tissue
Another characteristic sign of age-related changes is a decrease in the density of the bone tissue structure, expressed in a reduction in height, as well as the manifestation of excessive mobility of elements of the dentition. Jaw osteoporosis is considered a common pathology, affecting patients over 50 years of age. In addition, weakening of bone tissue leads to adentia - tooth loss - which results in incorrect distribution of the chewing load, leading to atrophy.
Negative processes also affect the soft tissues of the oral cavity. Gum recession, as a rule, is the result of the development of periodontal pathologies, genetic predisposition, non-compliance with medical recommendations and the presence of bad habits. Ultimately, age-related changes lead to complete tooth loss, requiring surgical dental treatment. At the same time, premature adentia can be avoided by regular visits to the doctor, which include preventive and physiotherapeutic procedures, as well as the restoration of individual lost or destroyed units.
How to treat a dental cyst
If a cyst appears in a tooth, what should you do? At the first signs of pathology, you should seek help from a doctor. The specialist will listen to complaints, conduct an examination of the oral cavity, and refer you for an X-ray examination. Treatment tactics depend on the extent of the inflammatory process.
Conservative methods
Therapeutic treatment of the disease is permissible in the initial stages, when the size of the cavity does not exceed 5 - 8 mm. Another prerequisite is good patency of the root canal, under which the cyst is located. General scheme of therapeutic treatment:
- Hard tooth tissues are prepared.
- Expand the entrances to the canal.
- The pulp is removed.
- Expand the lumen of the canal.
- Antiseptic and medicinal treatment of cavities is carried out.
- Temporary filling with dental paste, which accelerates the restoration of damaged tissue.
Treatment is long-term, taking from several months to 1 - 2 years. The patient periodically visits the doctor for follow-up examinations and repeated medicinal treatments. To suppress the growth of bacterial flora, a course of antibiotic therapy is usually prescribed. If control X-rays confirm the success of treatment, then a permanent filling is installed.
Surgical intervention
The operation is performed if the tooth formation is large, located in a hard-to-reach place, therapeutic treatment has not given a positive result, etc. Invasive intervention can be carried out according to different protocols
Cystectomy
Operation cystectomy - removal of the tumor along with the damaged root segment. This is a tooth-saving procedure. It is performed in the presence of a small tumor (extending no more than 2 teeth). How to remove a cyst on the root of a tooth:
- administration of local anesthetic;
- cut the gum above the formation;
- gain access to the capsule;
- remove the tumor;
- in case of union with the root, resection of its apex is performed;
- a bone-restoring drug is placed inside the resulting cavity;
- stitches are placed.
In the postoperative period, the patient is prescribed drug therapy.
Hemisection
Used on multi-rooted teeth. During the intervention, the destroyed root is amputated along with part of the crown and the capsule is removed. The cavity is filled with a polymer composition, the upper part is expanded with a composite material or prosthetic crown.
Cystotomy
The operation consists of resection of the anterior wall of the cyst. The contents of the capsule are pumped out through the formed hole, which eliminates internal pressure. This leads to a gradual reduction of the cavity. The manipulation is low-traumatic, but requires careful postoperative care.
Tooth extraction
Tooth-preserving operations cannot be used in all cases. In some clinical situations, it becomes necessary to remove a tooth. Indications for such a decision may include:
- significant size of education;
- the presence of an extensive zone of bone destruction around the segment;
- tumor growth into the maxillary sinus;
- other methods did not work.
After surgical treatment, the doctor gives recommendations on oral care in the postoperative period. If you ignore the dentist's advice, after removal of a dental cyst, adverse consequences are possible: wound infection, bleeding, relapse.
DEVELOPMENT AND STRUCTURE OF TEETH
There are 32 permanent teeth (dens permanens) in the oral cavity of an adult. In each half of the jaw (right or left) there are 2 incisors (dens incisius), 1 canine (dens caninus), 2 premolars, or small molars (dens praemolaris), and 3 molars, or large molars (dens molaris). The 3rd large molar is called the wisdom tooth (dens sapientiae).
In the oral cavity of a 6-7 year old child there are 20 primary teeth (dens deciduus). Each half of the jaw has 2 incisors, 1 canine and 2 large molars.
The tooth consists of a crown (corona dentis), rising above the gum; neck (cervix dentis), covered with gum; root (radix dentis), located in the alveolar process of the jaw.
The tooth includes hard and soft tissues. Hard tissues include enamel (enamelum), dentin (dentinum) and cement (cementum), while soft tissues include pulp (pulpa dentis).
The tooth is held in the socket of the alveolar process of the jaw with the help of a supporting (ligamentous) apparatus, including cement, periodontium and the wall of the socket. Some scientists (L.M. Tsepov) do not classify cement as a supporting apparatus of the tooth.
The development of teeth (odontogenesis) undergoes 3 stages: 1) the formation of the dental plate and the formation of tooth germs; 2) differentiation of tooth germs; 3) histogenesis.
1st stage
begins at the 6-7th week of embryogenesis with the formation of the vestibular plate. This plate is formed as a result of the ingrowth of epithelium into mesenchyme along the edge of the oral cavity. Then the vestibular plate splits into 2 layers, resulting in the formation of the vestibule of the oral cavity (vestibulum oris).
After this, a second strand of epithelium grows inward from the vestibular cavity. This is the dental plate (2 plates - upper and lower). From the inner surface of each plate, 10 epithelial outgrowths are formed - dental buds (gemma dentis). Mesenchyme grows into the dental buds - the dental papilla (papilla dentis). As the dental papilla grows from the dental bud, an epithelial dental organ (organum dentale epitheliale), or enamel organ, is formed. This organ has the shape of a double-walled bowl. The mesenchyme thickens around the enamel organ. This seal is called the dental sac (sacculus dentis).
As a result of the 1st stage of tooth development, a tooth germ is formed. It consists of 3 components: the dental organ, the dental papilla and the dental sac.
2nd stage
begins with the differentiation of the components of the tooth germ.
The differentiation of the dental organ (enamel organ) is characterized by the appearance of 3 layers.
The 1st layer is the internal epithelium (epithelium dentale internum), adjacent to the dental papilla. Its cells acquire a prismatic shape and are called enameloblastus, since enamel will then develop from them;
The 2nd layer is the outer epithelium (epithelium dentale externum), adjacent to the dental sac. Its cells have a flattened shape; after teething, they are partially reduced and partially fuse with the gingival epithelium;
The 3rd layer is the intermediate layer of the dental organ, located between the outer and inner layers. Its cells acquire a stellate shape as a result of the accumulation of fluid between them. This layer is called the pulp of the dental organ (pulpa organi dentis), from which the cuticle of the tooth is later formed.
The dental organ is connected to the dental plate using a neck. At the 3rd month of embryogenesis, the dental organ separates from the dental plate.
The differentiation of the dental papilla is that it increases in size and protrudes deeper into the dental organ. Blood vessels and nerve fibers grow into the dental papilla. On its surface, mesenchymal cells differentiate into preodontoblasts, or predentinoblasts. Dentin will later develop from these. Mesenchymocytes of the central part of the dental papilla differentiate into connective tissue cells of the future dental pulp.
The differentiation of the dental sac is manifested in the fact that it is divided into 2 layers: 1) internal and 2) external. Later, cementum will develop from the inner layer, and periodontium will develop from the outer layer.
Stage 3 (histogenesis)
includes:
1) dentinogenesis, or dentin development (dentinogenesis);
2) pulp development;
3) enamelogenesis, or development of enamel (enamelogenesis);
4) development of cementum and periodontium.
Dentinogenesis
begins in the 4th month of embryogenesis. Predentinoblasts of the dental papilla differentiate into dentinoblasts (dentinoblastus). Dentinoblasts have an elongated shape, contain an oval or round nucleus, the cytoplasm contains the Golgi complex, granular ER, mitochondria and the ALP enzyme. Processes extend from dentinoblasts. The process facing the dental papilla is called central.
Dentinoblasts produce collagen molecules, from which collagen fibers are polymerized, and the cementing substance predentin (glycoproteins, phosphoproteins, proteoglycans and phosphorins). Initially, collagen fibers have a radial direction. This is mantle predentin. When the thickness of predentin reaches 40-80 microns, collagen fibers acquire a tangential (longitudinal) direction, and pulpal predentin is formed.
As dentinoblasts deposit predentin substance, they move further and further from the surface to the center, but the ends of their peripheral processes remain in place, and the processes themselves lengthen. Predentin forms around the processes. Thus, the processes end up in the tubules, which are called dentinal. The resulting predentin, composed of organic matter, is a soft substance that can be cut with a knife. In order for predentin to become a solid substance - dentin, it is necessary to deposit salts in it (mineralization).
Mineralization
predentin is carried out in the 5th month of embryogenesis with the participation of alkaline phosphatase, under the influence of which glycerophosphate in the blood is broken down into phosphoric acid and monosaccharides. Phosphoric acid combines with calcium to form calcium phosphate, which is deposited in predentin to form dentin.
During the mineralization of predentin, numerous foci appear in it, in which crystals of mineral salts are deposited. These lesions increase in size and turn into globules (balls). As the globules grow, they merge, and the predentin becomes mineralized and hard. This method of mineralization is called globular.
However, some predentin remains unmineralized. Along the periphery of the developing tooth crown, non-mineralized areas remain, which are called interglobular spaces.
In addition, the part of predentin adjacent to the pulp also does not undergo mineralization;
called pulpal predentin
. Sometimes these areas are called non-calcified pulpal dentin.
Dental pulp development
begins simultaneously with the development of dentin. The central mesenchymal cells of the dental papilla differentiate into fibroblasts, which produce collagen molecules and other components of the intercellular substance of the pulp.
Enamelogenesis (enamel development)
begins after dentin formation.
At this time, the supply of nutrients from the dental papilla through the basement membrane to the cells of the inner layer of the dental organ (enameloblasts) stops, since a layer of dentin appears between the enameloblasts and the vessels of the dental papilla. In this regard, nutrients begin to flow to the enameloblasts from the intermediate layer (pulp) of the dental organ. This leads to the fact that the nucleus from the basal part of the enameloblasts, the Golgi complex and the cell center move to the apical part of the cells. Therefore, the apical part of the enameloblasts turns into the basal, and the basal - into the apical, directed towards the dentin. This is called inversion.
Thus, the formation of dentin provokes the inversion of enameloblasts, and after the inversion, the formation of enamel begins.
On the granular ER of enameloblasts, a protein begins to be synthesized, the granules of which move to the apical part of the cell and form the cuticular plate. As the number of granules in the cuticular plate increases, this plate lengthens and turns into a pre-enamel prism. The more the length of the prism increases, the shorter the anameloblasts become and the further they move to the periphery. After the formation of pre-enamel prisms, enamel mineralization begins.
Simultaneously with the formation of enamel, resorption of the dentin surface occurs, which therefore becomes uneven (scalloped), due to which the enamel is firmly connected to the dentin.
Cementogenesis (development of cement)
occurs in the 6-7th month of a child’s life, when baby teeth begin to erupt and their roots begin to develop.
The structure of the tooth.
Enamel (enamelum) covers the crown and partially the neck of the tooth. The greatest thickness of enamel is on the chewing surface (up to 3.5 mm). Enamel is the hardest tissue in the human body. It consists of 3-4% organic substances and 96-97% salts of calcium phosphate, calcium carbonate and calcium fluoride.
The structural unit of enamel is an enamel prism . Enamel prisms in their longitudinal section have an S-shape, in a transverse section - multifaceted, convex-concave, etc. The prisms are arranged in bundles almost perpendicular to the surface of the dentin. The prism consists of an organic matrix, represented by a network of the finest fibers, and salt crystals. Between the prisms there is a less calcified adhesive substance.
On a longitudinal section of a tooth, Retinus lines , which in a cross section have the shape of rings. The existence of these lines is explained by periodic weakening of mineralization, as well as forceful effects on the tooth during chewing. In addition, dark and light Schräger stripes . The presence of these stripes is explained by the fact that when grinding the tooth, some bundles of enamel prisms were cut perpendicularly, others - longitudinally.
The enamel contains enamel spindles (fusus enameli), enamel bundles (fasciculus enameli) and enamel plates (lamina enameli).
Enamel spindles
- these are the sites of penetration of dentinal tubules into the enamel. Nutrients enter the enamel through the enamel spindles from the dentinal tubules.
Enamel bundles
- these are narrow strips of weakly mineralized enamel, starting at the border with dentin and not reaching its surface.
Enamel plates
- these are narrow strips of weakly mineralized enamel, starting at the border with dentin and ending on its surface.
The presence of enamel bundles and enamel plates weakens the structure of the enamel, since bacterial toxins and bacteria enter the enamel through these bundles and plates, which destroy it.
The strength and chemical composition of enamel depend on metabolism in the body. Water, ions, amino acids, glucose and other substances can penetrate through the enamel. These substances come from saliva. Saliva affects the permeability of enamel. The permeability of enamel increases under the influence of acids, parathyrine, alcohol and with a lack of calcium, fluorine, and phosphorus salts in food. Enamel is connected to dentin through interdigitation.
Cuticle enamel
(cuticula enameli) is a thin organic plate covering the enamel. The cuticle develops from the pulp of the dental organ. The cuticle quickly wears off on the chewing surface and remains only on the lateral surface of the enamel. The cuticle protects the enamel from the harmful effects of various chemicals.
Dentin (dentinum) consists of the main substance in which the dentinal tubules (tubulus dentinalis) pass. The composition of dentin includes 28% organic substances (mainly collagen) and 72% salts (calcium phosphate, magnesium phosphate and calcium fluoride). There are 2 layers in dentin: 1) the outer mantle, in which the collagen fibers are located radially, and 2) the inner pulpal layer, in which the collagen fibers are located tangentially (longitudinally).
In the peripheral part of the dentin of the crown and root of the tooth there are non-calcified areas. In the crown, these areas are relatively large and are called interglobular spaces, in the root area they are small and are called the granular layer of Tomes
. Interglobular spaces take part in the metabolism of dentin.
The inner part of the pulpal dentin does not contain salts (not mineralized) and is called a strip of predentin,
or
uncalcified dentin.
Dentinal tubules
start from the pulp cavity, have a radial direction and end on the surface of the dentin. Some tubules penetrate the enamel (enamel spindles). In the pulpal dentin, the density of dentinal tubules is 75,000 per 1 mm2, in the mantle - 15,000-30,000 tubules. In the crown of the tooth, the dentinal tubules branch weakly, in the dentin of the root - strongly.
The wall of the dentinal tubules consists of peritubular dentin, which differs in that the collagen fibers in it have a circular direction and are richer in mineralization. Dentin located between the dentinal tubules is called intertubular (intertubular).
The dentinal tubules contain the peripheral processes of dentinoblasts and contain fluid. Dentinal tubules take part in metabolism and have trophic significance.
Dentin contains weakly mineralized areas in the form of thin stripes. These sections are called Owen's lines . On a longitudinal section of a tooth, Owen's lines have a tangential direction, and on a transverse section, they have a circular direction.
The dentin surface facing the enamel has interdigitation that promotes its strong connection with the enamel.
Secondary dentin
is formed by dentinoblasts after tooth eruption in a strip of non-calcified pulpal dentin. Secondary dentin includes: 1) replacement dentin and 2) denticles.
Replacement dentin
produced by dentinoblasts when the outer surface of dentin begins to deteriorate. 2 weeks after dentin destruction, newly formed predentin appears. After another 2 weeks, this predentin undergoes mineralization. If the process of dentin destruction proceeds quickly, then replacement dentin does not have time to form and a defect occurs in the dentin.
Denticles
are formed by dentinoblasts in the dental pulp during inflammatory and dystrophic processes. There are denticles: 1) free, located in the pulp of the tooth; 2) parietal, adjacent to the wall of the pulp cavity; 3) interstitial, included inside the tooth wall.
Secondary dentin is characterized by an irregular arrangement of collagen fibers and dentinal tubules and an abundance of interglobular spaces.
Cement (cementum) covers the neck and root of the tooth, contains 30% organic and 70% inorganic substances (mainly calcium phosphate and calcium carbonate). There are 2 types of cement: 1) acellular, covering the neck and the part of the tooth root extending from the neck; 2) cellular, covering the apex of the tooth root.
Cell cement
similar to coarse-fibered bone. It contains cells - cementocytes (cementocytus) and multidirectional collagen fibers. Cementocytes are located in lacunae, from which tubules extend, connected to the same tubules or to dentinal tubules, through which the exchange of substances between cementum and dentin occurs. The tubules extending from the lacunae contain processes of cementocytes.
Acellular cementum
consists only of a cementing substance and collagen fibers directed radially and longitudinally. The radial fibers are embedded into the dentin with their inner ends, and the outer ends pass into the periodontal fibers and are embedded in the wall of the alveolar process of the jaw, forming a circular ligament of the tooth.
Dental pulp,
located in the pulp cavity of the crown and in the root canal of the tooth, it is a type of loose connective tissue. There are 3 layers in the dental pulp: 1) peripheral, adjacent to the wall of the pulp cavity; 2) intermediate, adjacent to the peripheral; 3) central.
Peripheral layer
The pulp is represented by dentinoblasts (dentinoblastocytus), which have a process shape, a length of about 20-30 µm and a thickness of 6 µm. The cytoplasm contains the Golgi complex, granular ER, mitochondria and sudanophil granules. Their peripheral process penetrates the dentinal tubule and takes part in metabolic processes and, possibly, in the perception of irritations. This is evidenced by the presence of acetylcholinesterase in the processes.
The intercellular substance of the peripheral layer of the pulp includes collagen fibers, glycosaminoglycans, proteoglycans, glycoproteins and other substances inherent in the intercellular substance of loose connective tissue.
Intermediate layer of pulp
represented by immature collagen fibers and poorly differentiated cells capable of differentiating into dentinoblasts.
Central layer of pulp
consists of fibroblasts, macrophages and adventitial cells, collagen and reticular fibers. The function of the pulp is trophic.
Periodontium is a dense connective tissue that belongs to the supporting (connecting) apparatus of the tooth and consists of collagen fibers. The inner end of these fibers is embedded in the cement of the neck and root of the tooth, and the outer end is embedded in the jaw bone. The periodontium contains layers of loose connective tissue through which blood vessels pass. The periodontal collagen fibers in the area of the tooth neck form a circular ligament.
The periodontium performs 2 functions: 1) holds the tooth root in the socket; 2) participates in tooth trophism thanks to blood vessels passing through layers of loose connective tissue.
The periodontium includes periodontitis, the bone of the alveolar socket of the jaw and the gum.
Eruption of baby teeth. Development of root and cementum. Milk teeth begin to erupt at the 6-7th month of a child’s life. Before eruption, pulp accumulates in the tooth crown, resulting in an increase in intrapulpal pressure, under the influence of which the tooth crown begins to move to the surface of the gum. The incisors erupt first, then the canines, then the molars.
The process of teething is influenced by nutrition, diseases, the presence of vitamins and other factors. After the crown of the tooth has erupted, its root begins to develop.
Root development
begins from the moment of teething.
If the tooth is single-rooted (incisor, canine), then the lower edge of the epithelial dental organ begins to grow into the mesenchyme. This growing edge is called the “Hertwig root epithelial sheath.”
Hertwig's vagina has the shape of a tube. Its growing edge is slightly tucked inward.
Peripheral mesenchymal cells adjacent to the inner surface of Hertwig's sheath differentiate into dentinoblasts, which begin to produce predentin of the tooth root, followed by its calcification.
The central mesenchymal cells differentiate into fibroblasts, which produce components of the intercellular substance of the tooth root pulp.
If the tooth is double-rooted (premolar), then from the edge of the enamel organ 2 processes grow towards each other. After the fusion of these processes, 2 holes are formed in the Hertwig sheath, and from each of these holes a new Hertwig sheath grows, inside which dentin and pulp of the tooth root are formed.
If a tooth has 3 roots (molars), then 3 processes extend from the lower edge of the enamel organ. After the fusion of these processes, 3 openings are formed, from each of which one Hertwig’s vagina extends.
Development of cement
begins with the fact that the mesenchymal cells of the inner layer of the dental sac differentiate into cementoblasts, which destroy the epithelium of the Hertwig vagina. As a result of contact of cementoblasts with dentin of the root and neck of the tooth, cementoblasts are activated and begin to produce the intercellular substance of cement (collagen, glycosaminoglycans, proteoglycans and other substances).
As the tooth root grows, cementoblasts move to its apex, wall themselves with cement and turn into process-shaped cementocytes located in the lacunae. Therefore, the cement in the area of the apex of the tooth root, in which the cementocytes are located, is called cellular cement. The cement of the neck of the tooth and the base of its root does not contain cementocytes, and is therefore called acellular cement.
Periodontal development
occurs due to the mesenchymal cells of the outer layer of the dental sac, which differentiate into fibroblasts that produce collagen protein and other components of the intercellular substance of connective tissue.
The replacement of baby teeth and the eruption of permanent teeth begins in the 6-7th year of a child’s life. In the 5th month of embryogenesis, permanent incisors and first molars are formed, then premolars and canines; second molars - in the 1st year, third molars - in the 4th-5th year of the child’s life.
Permanent teeth, which have milk precursors (incisors have incisors, canines have canines, premolars have molars), are laid below and behind the rudiments of milk teeth and are located in the same cavity with them. Later, the rudiments of permanent teeth are separated from the milk teeth by a bone septum.
As the dental plate lengthens, the rudiments of permanent molars appear on it, which do not have milk predecessors.
Eruption of permanent teeth that have deciduous predecessors
characterized by the fact that in the crown of a permanent tooth the amount of pulp increases, which presses on the crown, promoting its advancement towards the gum surface. At this time, osteoclasts destroy the bone septum between the permanent tooth germ and the root of the baby tooth. As the crown moves toward the gum surface, dentinoclasts and cementoclasts destroy the root of the baby tooth. At the moment when the root of the baby tooth is completely destroyed, the crown of the baby tooth, practically not held in place by anything, is easily pushed out by the crown of the permanent tooth.
The first to erupt after the first molar are the permanent incisors, then, within 9-14 years, the canines and premolars (small molars).
Eruption of permanent large molars (molars),
having no milk predecessors, is carried out in exactly the same way as the eruption of milk teeth, but only at a later date and after the lengthening of the dental plate. The first molar erupts at the 6-7th year of the child’s life, the second molar at the 9-14th year and the third molar at the 20-25th year.
Vascularization of teeth
carried out by the branches of the maxillary artery, penetrating through the main and additional openings in the apical part of the tooth root. In the dental pulp, the arteries branch into many anastomosing capillaries, which flow into a vein that leaves the pulp cavity through the same openings in the tooth root. The pulp contains lymphatic capillaries and small lymphatic vessels.
Blood flow in the pulp vessels is influenced by temperature and changes in mechanical pressure during chewing of food.
Innervation of the tooth
carried out by branches of the trigeminal nerve, the fibers of which end in receptors. There are unmyelinated nerve fibers ending with effectors on pulp vessels.
There is evidence that sensory nerve fibers penetrate into the initial sections of the dentinal tubules. These fibers perceive painful stimulation that occurs under the influence of pressure on them from the fluid located in the dentinal tubules. It is possible that painful stimuli are perceived by the processes of dentinoblasts, as evidenced by the presence of acetylcholinesterase in these processes.
Age-related changes in teeth
characterized by the fact that the enamel and dentin on the chewing surface are erased. The enamel becomes dull, cracks appear on its surface, and mineral salts are deposited. In enamel, dentin and cement, the content of organic substances decreases and the amount of mineral compounds increases. As a result, the permeability of these tissues to water, ions, amino acids, enzymes, and glucose decreases. As the body ages, new dentin formation stops. Cement, on the contrary, grows.
The dental pulp atrophies in old age, and the nutrition of the dental tissues is disrupted due to sclerosis of the blood vessels. The number of dentinoblasts decreases, some of them turn into dentinocytes.
Regeneration
There is no tooth enamel observed, dentin regeneration is carried out due to the formation of secondary replacement dentin, carried out by dentinoblasts.